Downloaded 384 times


































































This document provides an overview of the history, definitions, classification, epidemiology and psychiatric disorders associated with epilepsy. It discusses how epilepsy was viewed in ancient times as a supernatural condition and outlines key developments in understanding including Hippocrates' view of it as a brain disorder. It defines terms like seizure, aura and epilepsy and classifies seizure types. Statistics on prevalence and risk factors for psychopathology in epilepsy are presented. Specific psychiatric conditions like depression, anxiety and inter-ictal psychosis are also examined.
The presentation introduces epilepsy through historical accounts, definitions, and stigma faced by patients.
Defines seizures and epilepsy; discusses the processes like epileptogenesis and terms related to seizures.
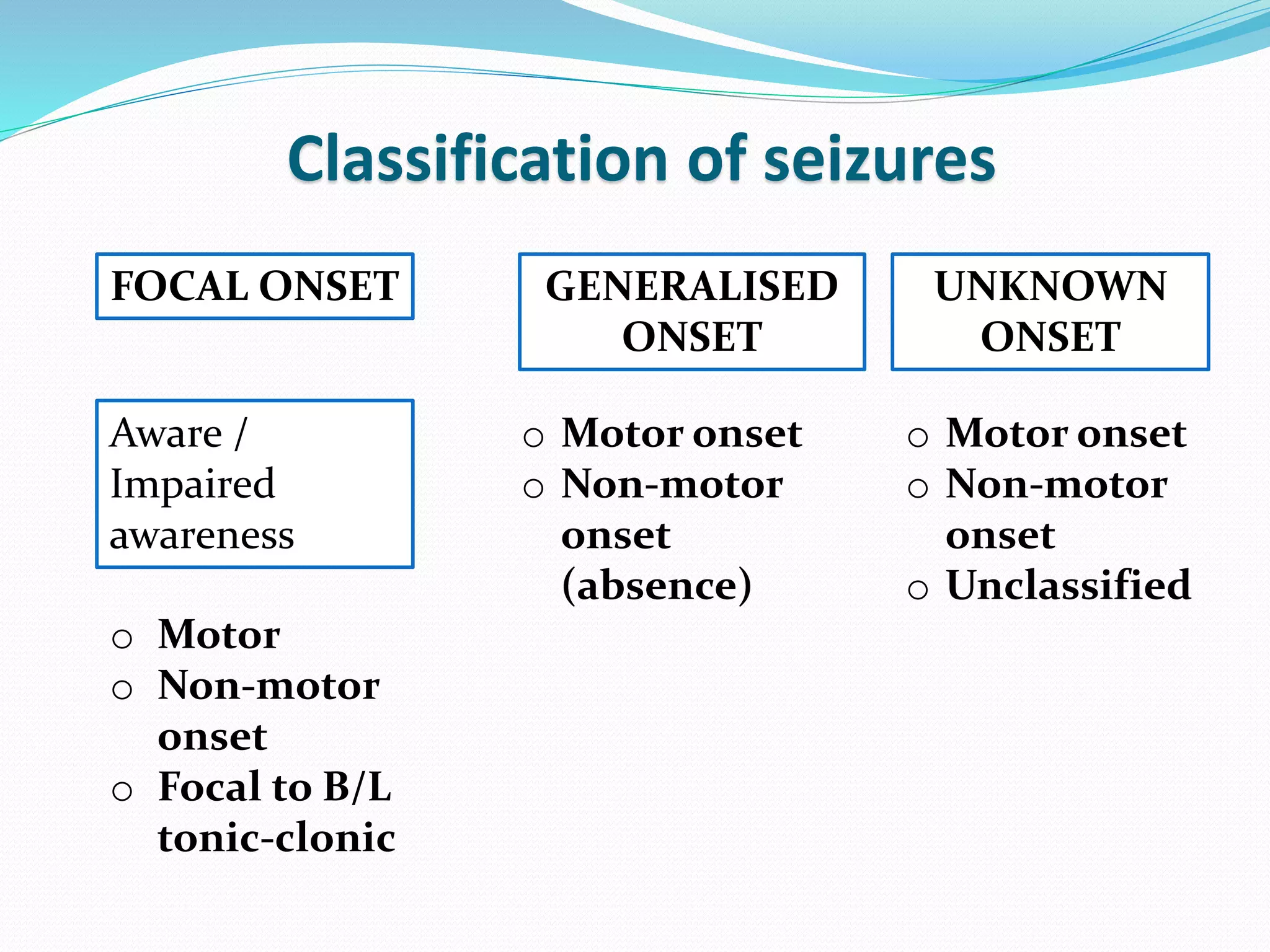
Categorizes epilepsy into generalized and focal seizures with specific types and syndromes described.
Highlights statistics on epilepsy prevalence globally and in India; discusses early onset and familial incidence.
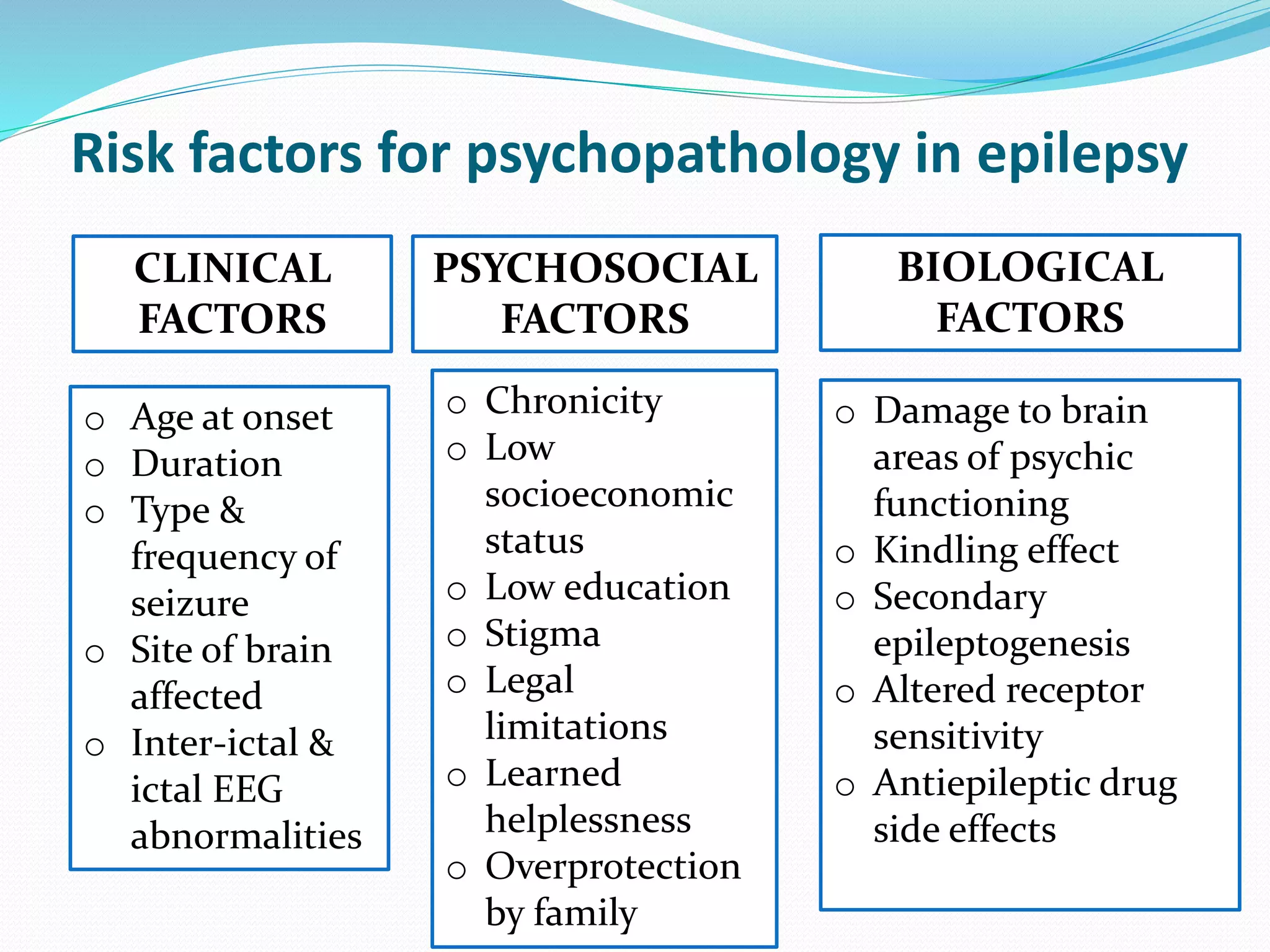
Details psychiatric disorders associated with epilepsy, particularly in patients experiencing seizures.
Examines psychiatric phenomena related to the timing of seizures including prodromes and postictal psychosis.
Explores non-epileptic seizures' characteristics and differentiates them from actual epileptic seizures.
Discusses the link between epilepsy and aggression, as well as cognitive functions impacted by the condition.
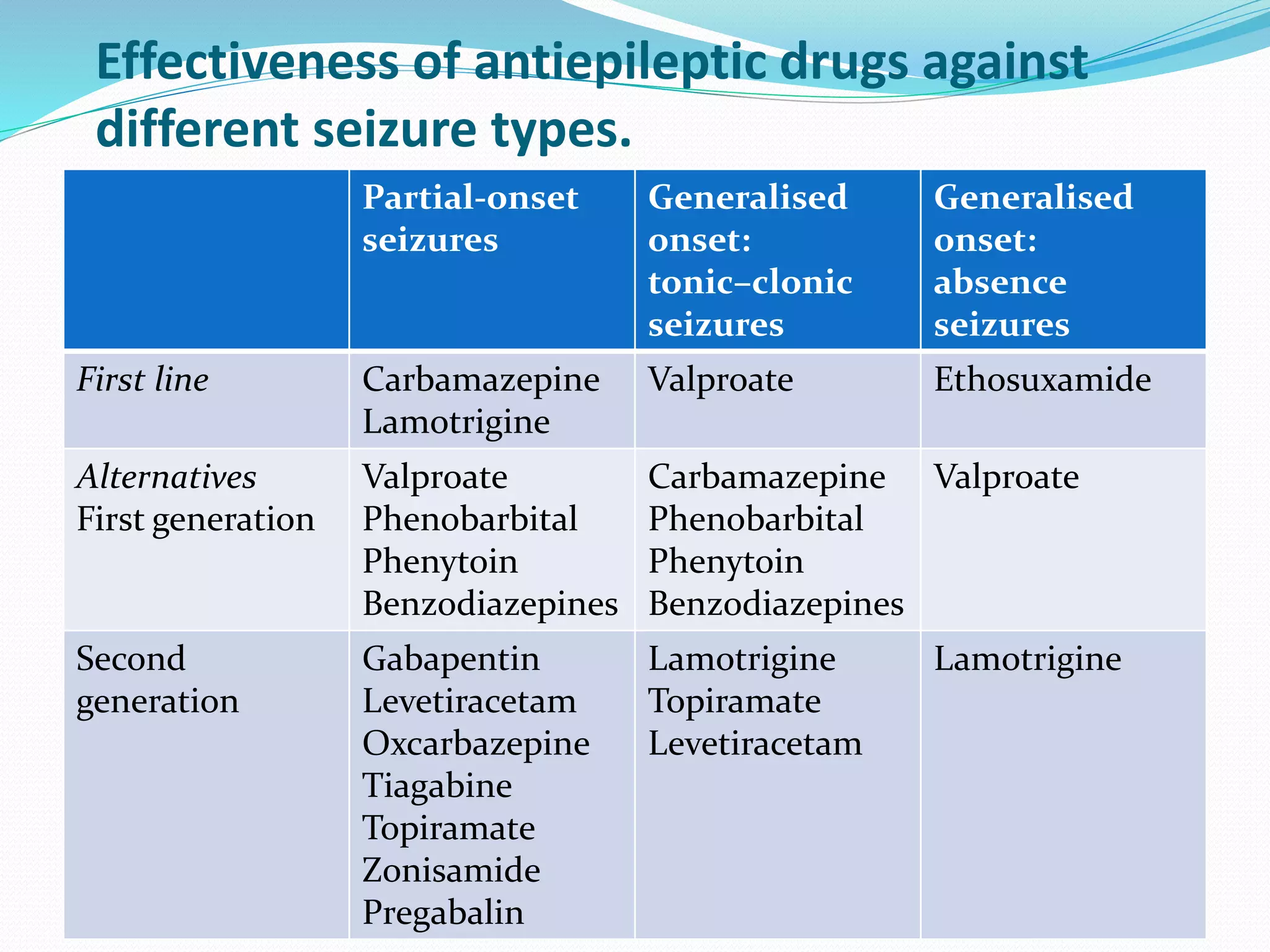
Presents the treatment options for epilepsy, including medications, surgery, and vagal nerve stimulation.Wraps up the presentation, listing references for further reading and research on epilepsy.


















![Neurocognitive Disorders [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/ncd2020v2-200526001756-thumbnail.jpg?width=640&height=640&fit=bounds)

























![Epilepsy[1].pptEpilepsyEpilepsy[1].pptEpilepsy](https://cdn.slidesharecdn.com/ss_thumbnails/epilepsy1-240412111639-e8fd8f7c-thumbnail.jpg?width=640&height=640&fit=bounds)































