Downloaded 172 times
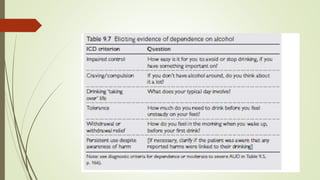

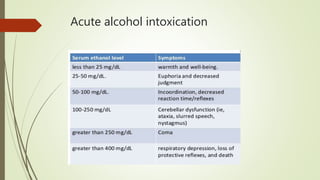

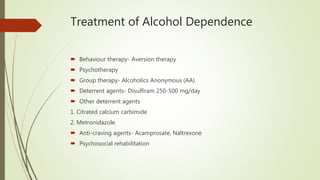
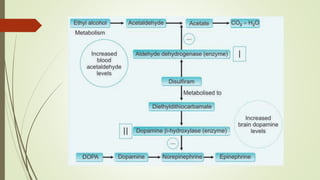


This document discusses alcohol use disorders and their treatment. It defines key terms like acute intoxication, withdrawal state, and dependence syndrome. It describes the major symptoms of alcohol withdrawal. It also outlines chronic health complications of alcohol use like Wernicke's encephalopathy and Korsakoff's psychosis. The document lists screening tools and treatments for alcohol dependence, including detoxification with benzodiazepines, vitamin supplementation, and approaches like psychotherapy, group therapy, and medications to reduce cravings or deter drinking.














































![Etoh[1]](https://cdn.slidesharecdn.com/ss_thumbnails/etoh1-140225215207-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)



















