Downloaded 115 times
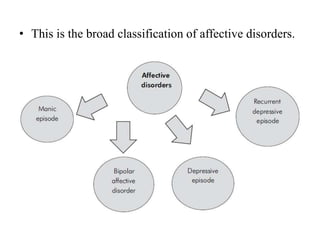

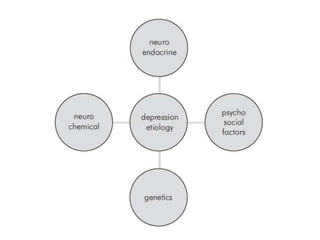



- Affective disorders include persistent mood disorders like depression that cause socio-occupational dysfunction. Depression is the most common mental disorder. - The document outlines depression and bipolar affective disorder, their diagnostic criteria, clinical features, management, and when to refer patients. Depression is a leading cause of disability and its early identification and treatment improves outcomes. Bipolar disorder involves episodes of mania or hypomania with or without depression.





































































![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)





