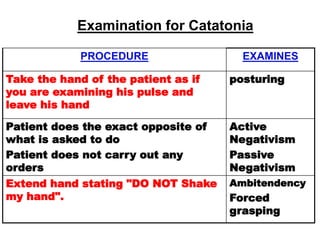
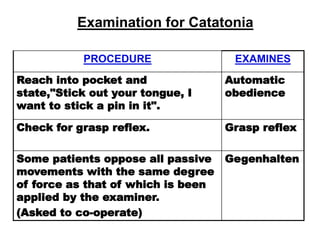
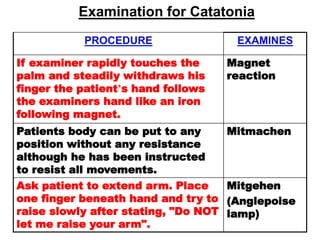
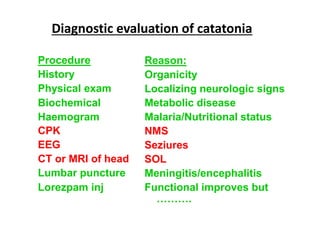
The document provides an overview of catatonia, a syndrome characterized by various motor and behavioral symptoms, with historical context and hypotheses regarding its causes, including neurological and psychological factors. It details distinguishing features, diagnostic criteria from DSM-IV and ICD-10, and compares psychiatric versus organic catatonia. Treatment options include lorazepam, electroconvulsive therapy, antipsychotics, and antidepressants, emphasizing the importance of addressing both primary and secondary causes.


































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
















