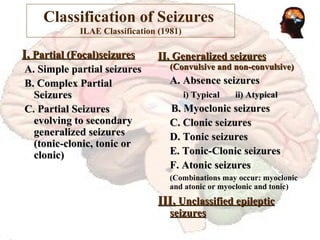
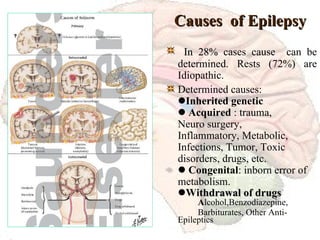
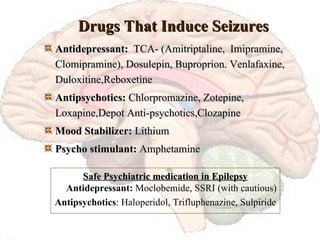
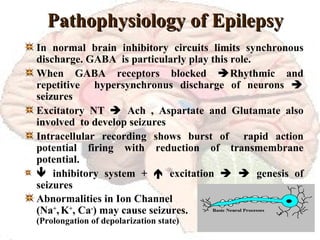
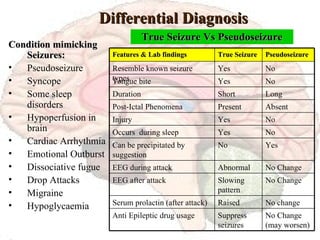
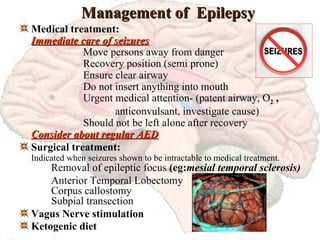
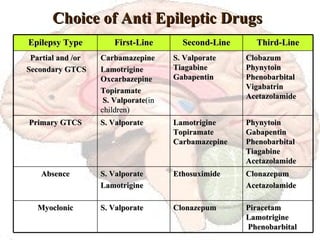
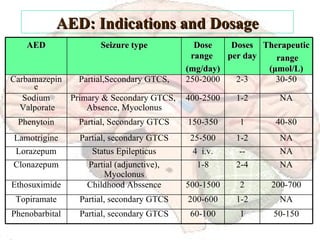
The document discusses the historical background, epidemiology, classification, causes, clinical presentation, diagnosis, and management of epilepsy. It emphasizes the advancements in treatment options, including both medical and surgical interventions, as well as the significant psychiatric comorbidities associated with the condition. Key findings highlight the prevalence rates and the importance of individualized treatment strategies in epilepsy care.
![Recent Advancements in Epilepsy Dr. Helal Uddin Ahmed Assistant Registrar National Institute of Mental Health [email_address]](https://image.slidesharecdn.com/epilepsy-1233773401615061-1/85/Epilepsy-an-overview-1-320.jpg)
![Recent Advancements in Epilepsy Dr. Helal Uddin Ahmed Assistant Registrar National Institute of Mental Health [email_address]](https://image.slidesharecdn.com/epilepsy-1233773401615061-1/75/Epilepsy-an-overview-1-2048.jpg)


![Recent Research and Achievements Drug treatments: Sodium valporate or Lamotrigin is chosen as first line treatments for Absence seizures and partial seizures. [BMJ vol 318 ] SANAD ( Standard and New Anti-epileptic Drugs ) study : Valporate is significantly better than Topiramate and Lamotrigine in treatment of idiopathic generalized seizures .[Lancet vol 369 March 2007] Surgery: In developing countries, in patients with Mesial TLE are feasible by a knowledgeable team consisting epileptologist, neurosurgeon, and technicians with using MRI and EEG. [Epilepsia 49(3):381-5.2008] In Benign Rolandic Epilepsy: Children with BRE demonstrated specific recognition impairments due to cortical auditory dysfunction. [Epilepsia, 49(6):1018-1026.2008]](https://image.slidesharecdn.com/epilepsy-1233773401615061-1/85/Epilepsy-an-overview-36-320.jpg)
![Recent Research and Achievements Seizure after Stroke: Overall incidence of seizures within 24 hours after stroke was 3.1%. Higher incidence seen in hemorrhagic stroke (8.4%). Seizures after stroke had higher mortality at 30 days after stroke .[ Epilepsia 49(6):974-981.2008] Akershus Study : Seizure free epilepsy patients on AED monotherapy improve neuropsychological performance after withdrawn the AED but a relative risk of seizures relapse 2.46, compared to those continuing medications. [Epilepsia 49(3):455-463.2008 ]](https://image.slidesharecdn.com/epilepsy-1233773401615061-1/85/Epilepsy-an-overview-37-320.jpg)



















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)













