Downloaded 1,226 times






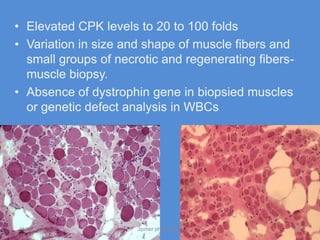

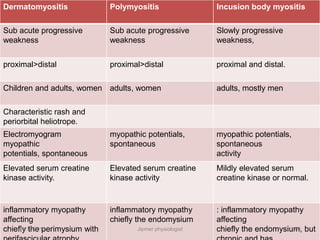
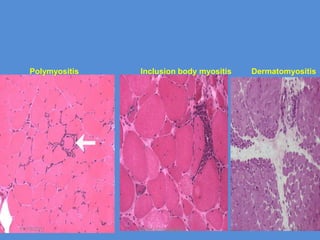
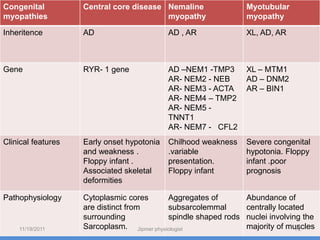




The document discusses neuropathies and myopathies, detailing their definitions, symptoms, classifications, and underlying causes. Neuropathies result from nerve damage impacting motor, sensory, and autonomic functions, with various etiologies including hereditary, metabolic, and toxic factors. Myopathies are neuromuscular disorders characterized by muscle weakness due to muscular fiber dysfunction and include several subtypes and clinical features.

































![28 [chapter 28 the reproductive system]](https://cdn.slidesharecdn.com/ss_thumbnails/28chapter28thereproductivesystem-170828134050-thumbnail.jpg?width=640&height=640&fit=bounds)











































