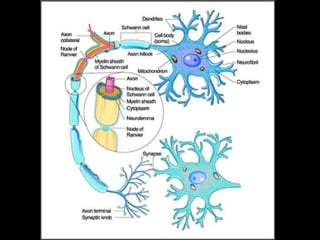
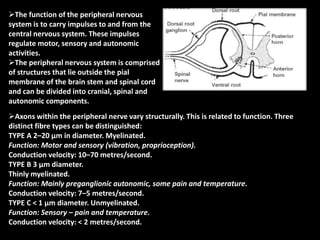
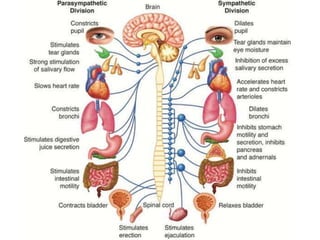
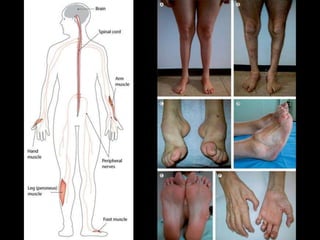
I. The peripheral nervous system carries signals between the central nervous system and the rest of the body. It has three main components - cranial, spinal, and autonomic. There are three main types of nerve fibers - A, B, and C - which differ in diameter, myelination, and function.
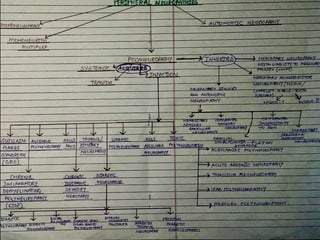
II. Peripheral neuropathies can be acquired through systemic diseases, trauma, infections, or inherited genetically. Common acquired neuropathies include diabetic neuropathy, Guillain-Barré syndrome, chronic inflammatory demyelinating polyneuropathy, and alcoholic neuropathy. Inherited forms include Charcot-Marie-Tooth disease and hereditary liability to pressure palsies.