Downloaded 174 times


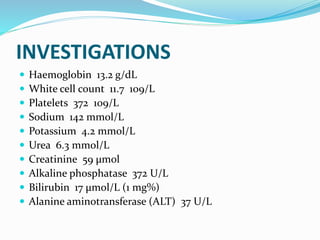


A 3-year-old boy presented with puffy eyes and edema. Examination found pitting edema, elevated heart rate, and proteinuria. Tests showed normal kidney and liver function. He was diagnosed with nephrotic syndrome based on his symptoms and urine protein level. Nephrotic syndrome is characterized by protein in the urine and symptoms of edema, low albumin, and high cholesterol or lipids. The majority of cases in children are idiopathic and due to minimal change disease. Treatment involves supportive care, steroids, and other medications depending on response and side effects.






























































































