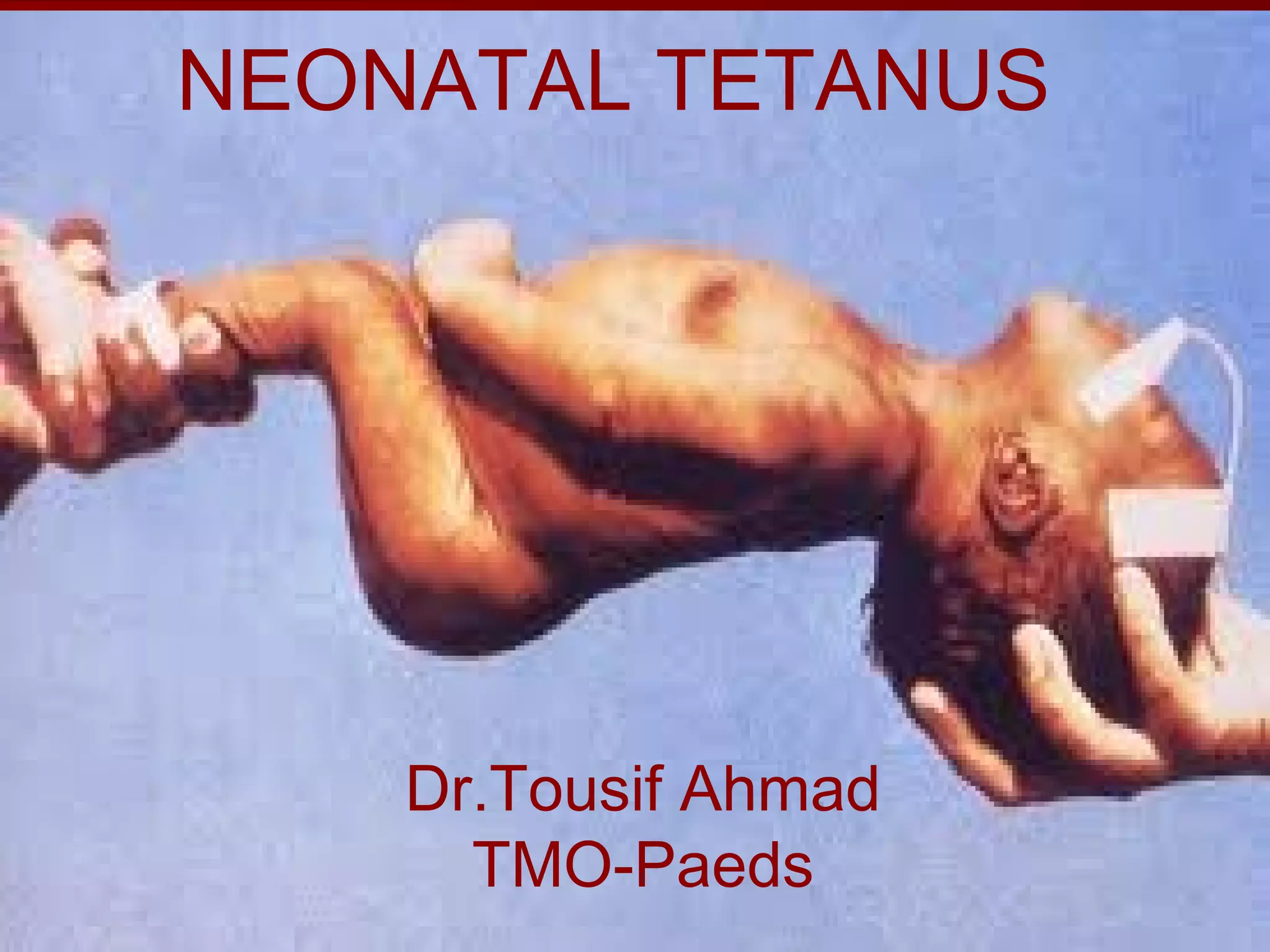
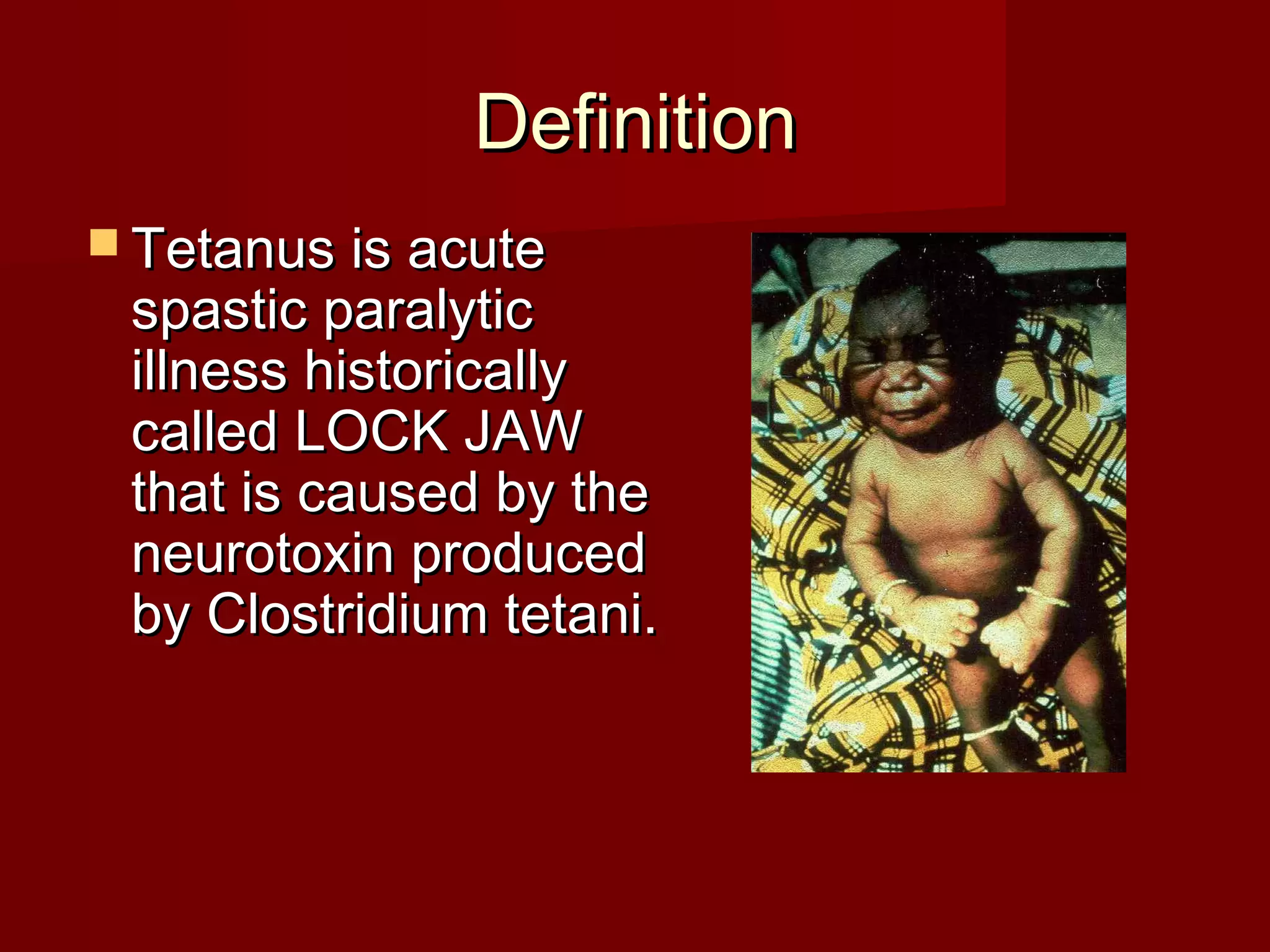
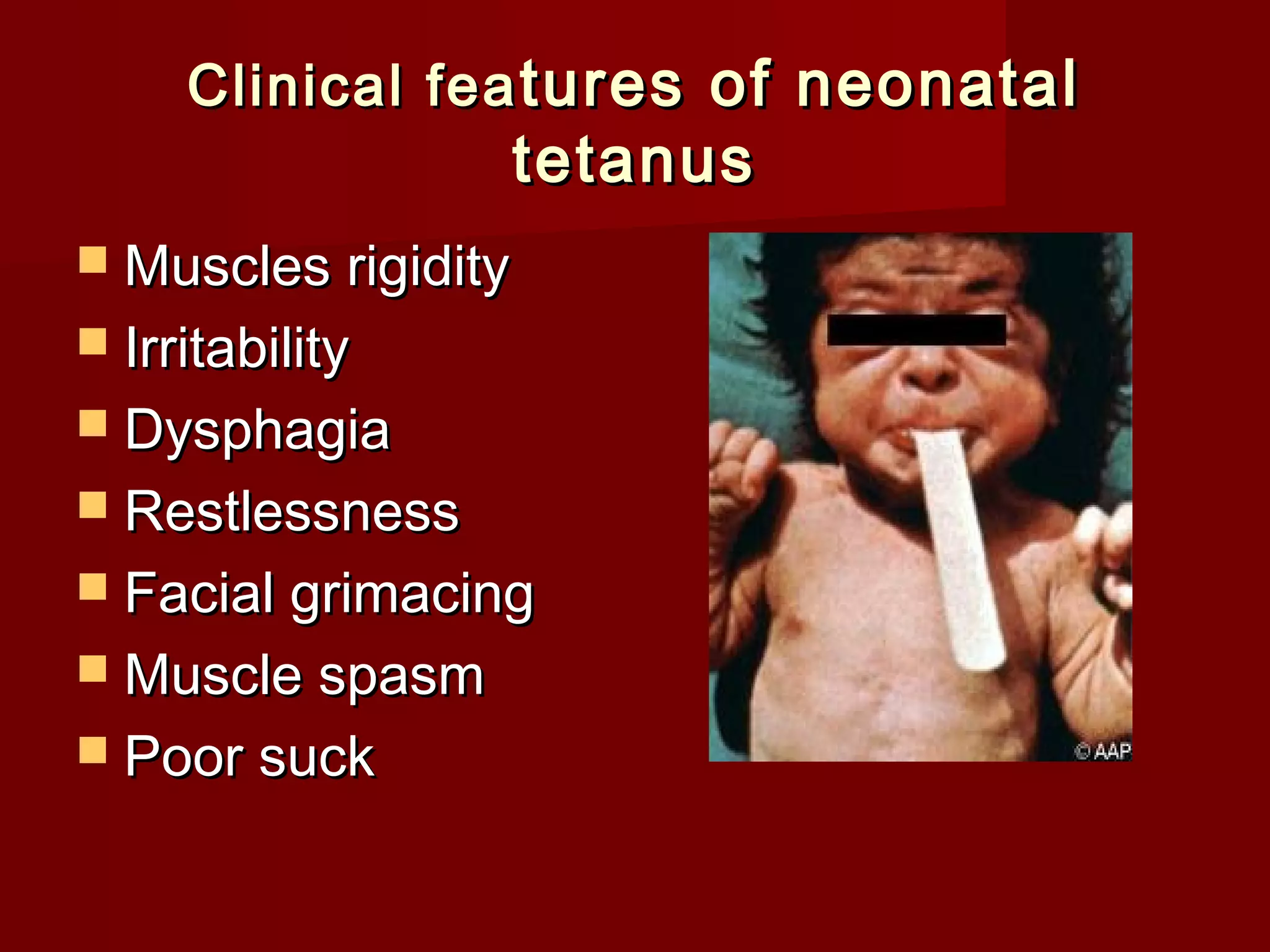
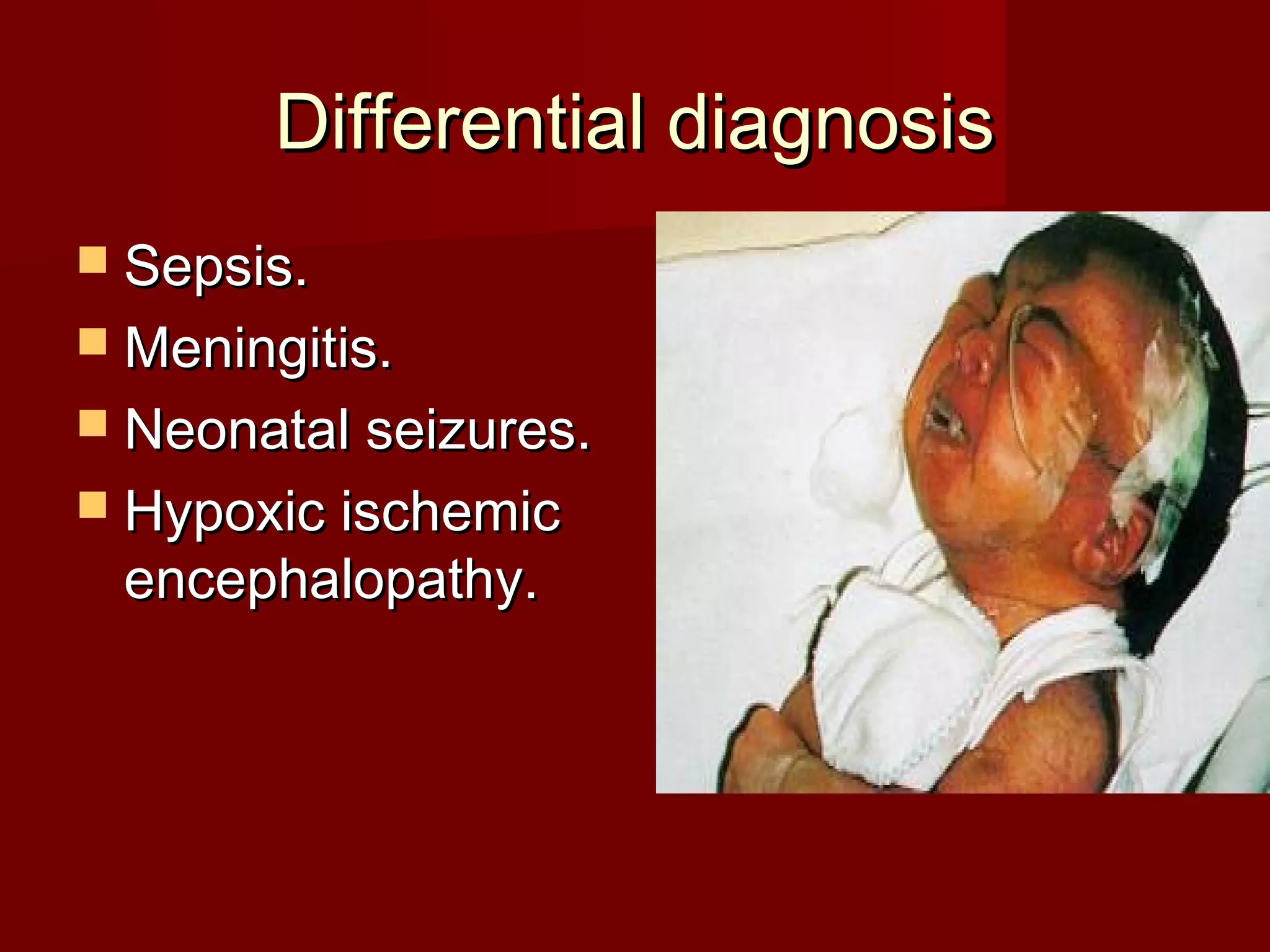
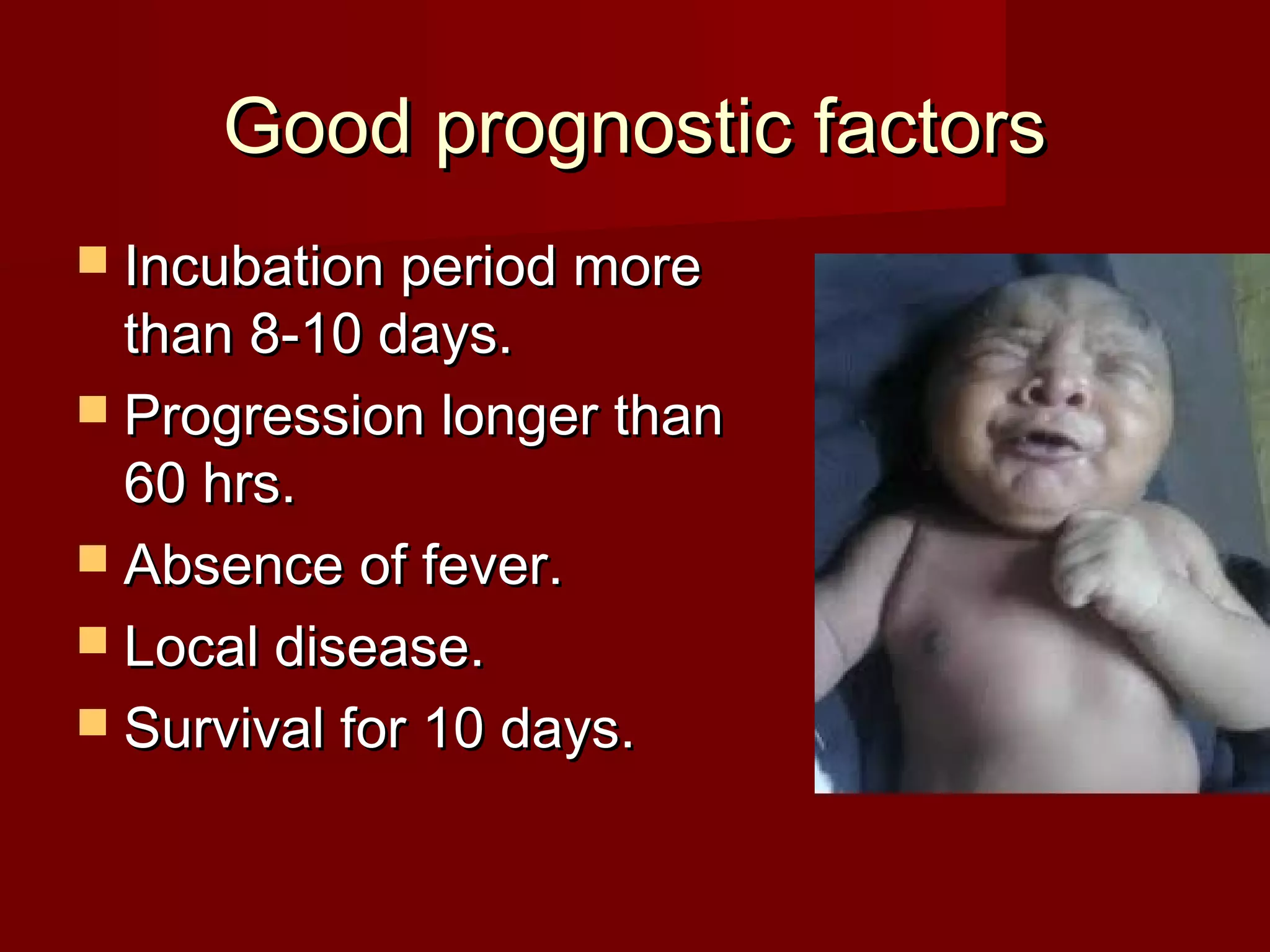
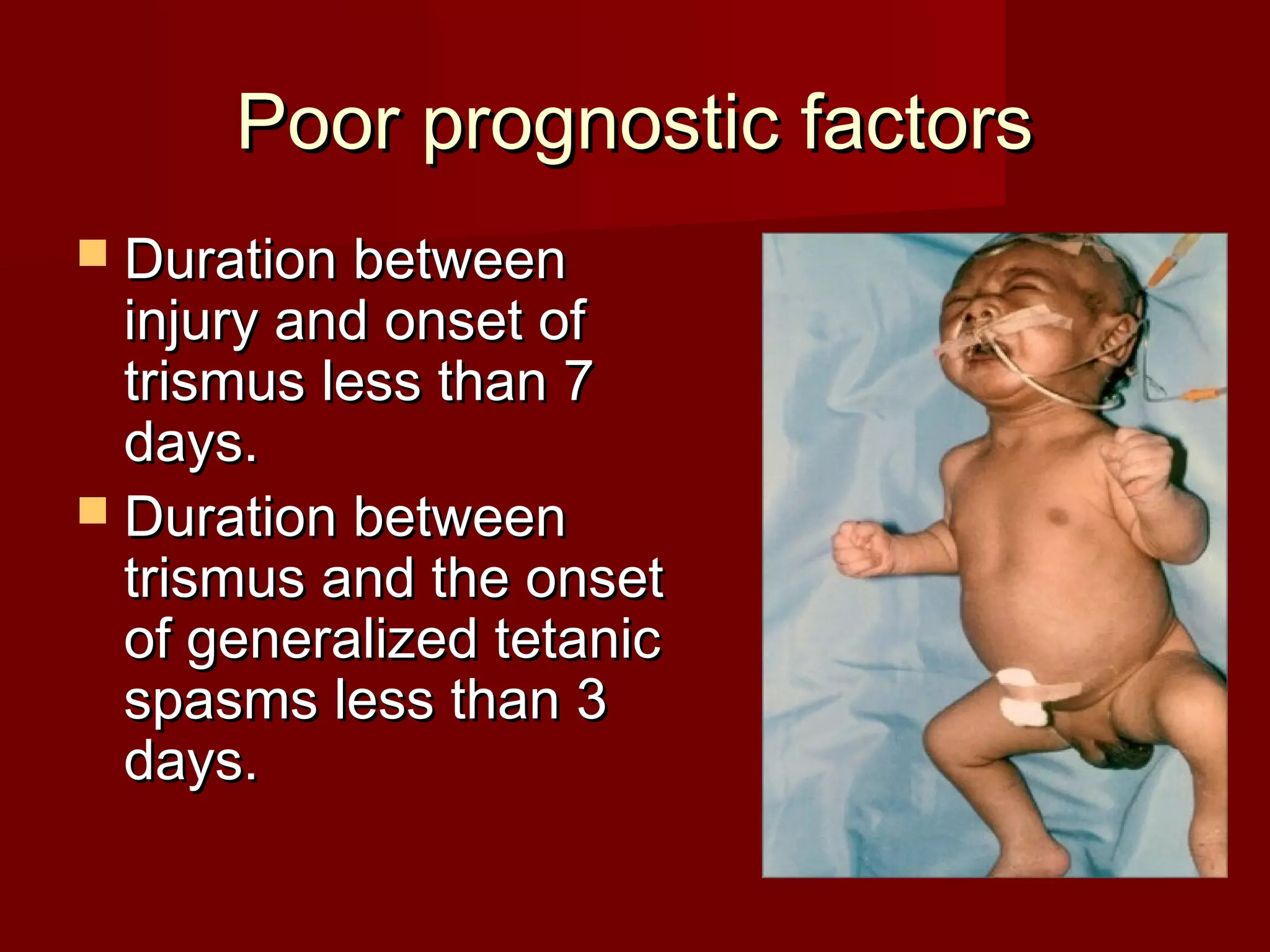


A 5-day-old newborn presented with generalized body stiffness, inability to suck, and fever. The baby was delivered at home by a traditional birth attendant, and the umbilical cord was cut with an unsterile instrument. On examination, the baby had generalized spasms triggered by stimuli, locked jaw, tense abdomen, and an infected umbilical cord. The diagnosis was neonatal tetanus. Neonatal tetanus results from infection of Clostridium tetani spores in the umbilical stump of newborns without protective immunity from unimmunized mothers. Management involves wound cleaning, antibiotics, antitoxin, sedation, feeding via NG tube, and supportive care






























































































