Downloaded 217 times



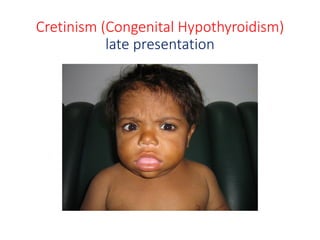
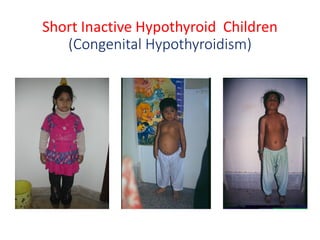
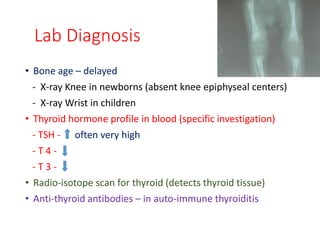
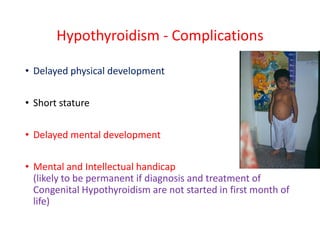
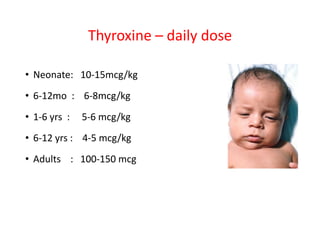
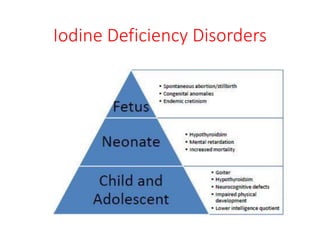


Hypothyroidism in children can be congenital or acquired. Congenital hypothyroidism is present from birth and is usually caused by thyroid dysgenesis or iodine deficiency in high-risk areas. It presents with poor feeding, constipation, large tongue, and delayed development. If not treated early with thyroxine replacement, it can cause intellectual disability. Acquired hypothyroidism develops later in childhood and may be caused by autoimmune thyroiditis, iodine deficiency, or rare genetic disorders. Hypothyroidism is diagnosed through clinical features, low thyroid hormone levels, and high TSH. Treatment involves lifelong thyroxine replacement to prevent complications of delayed growth and intellectual development