
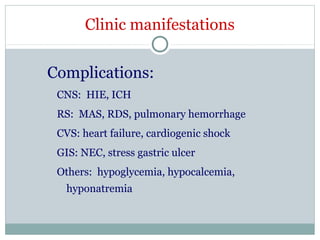
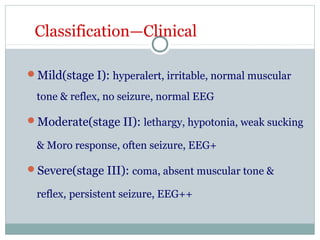
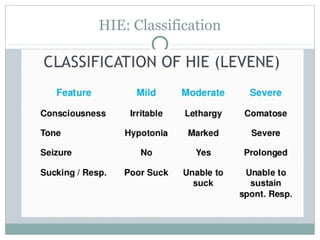
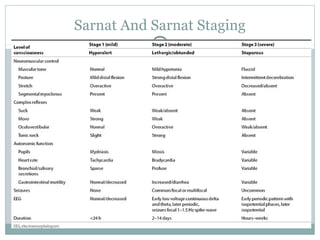


Clinically, more term babies suffered from hypoxic ischemic encephalopathy (HIE) than premature babies. However, pathologically, more premature babies suffered from HIE than term babies. The main clinical manifestations of HIE are symptoms of consciousness, including excitation symptoms like hyperalertness, irritability, and seizures, or depressing symptoms like coma and hypotonia. Management of HIE focuses on monitoring, controlling seizures, general supportive care, and recent advances like therapeutic hypothermia. The prognosis depends on the severity of brain damage and treatment, with mild or moderate cases often recovering completely but severe cases having a high risk of mortality or long-term complications.