Downloaded 1,086 times
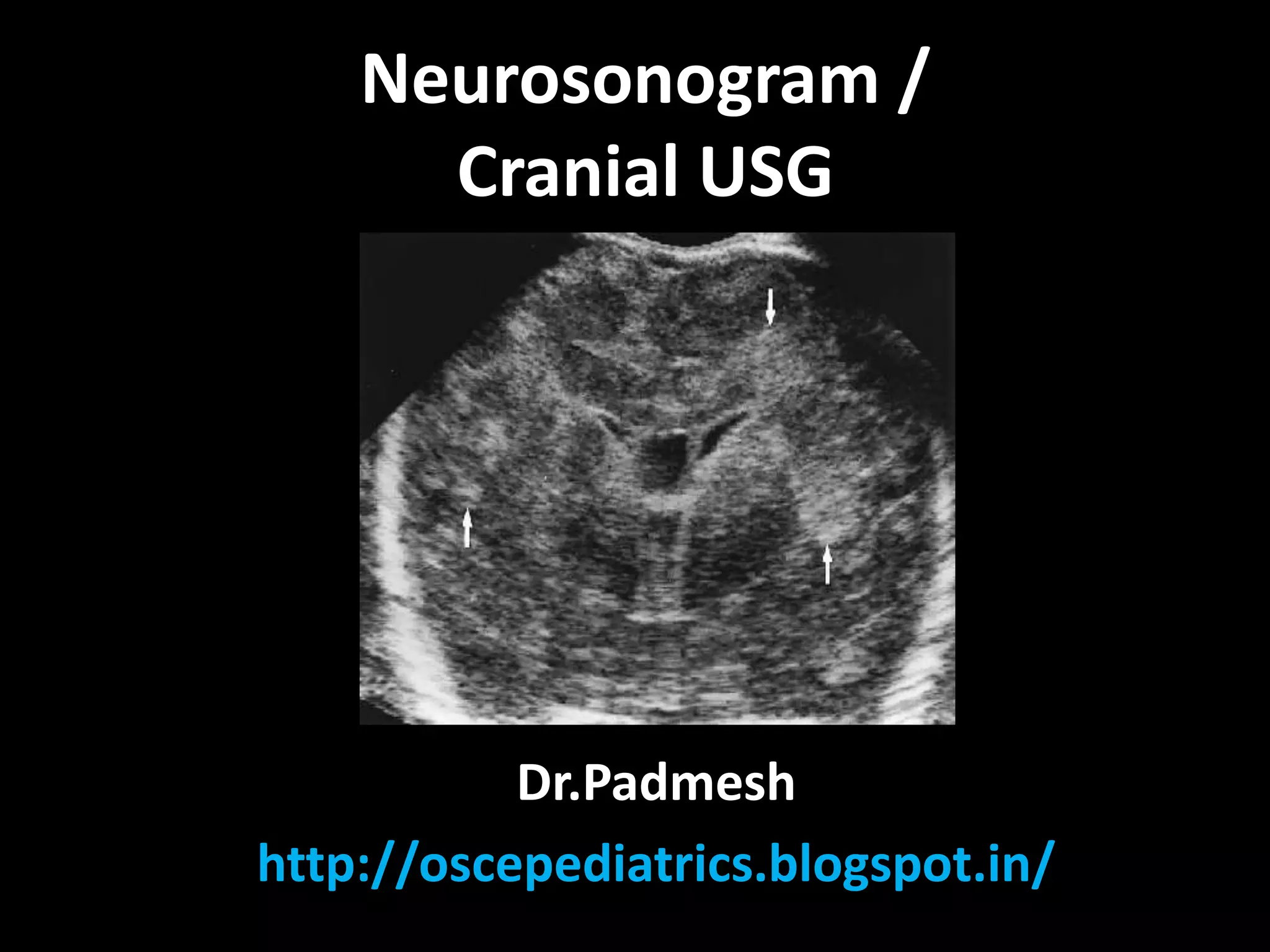

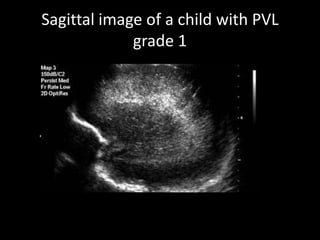
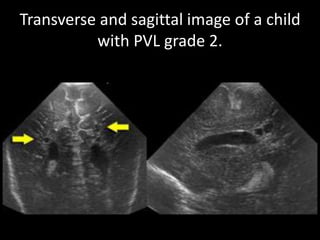
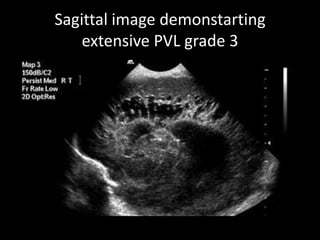
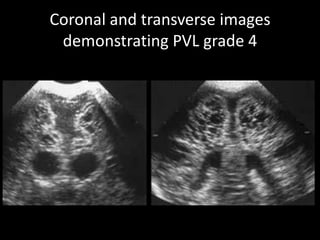
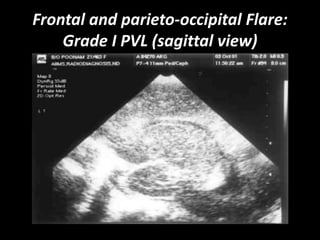
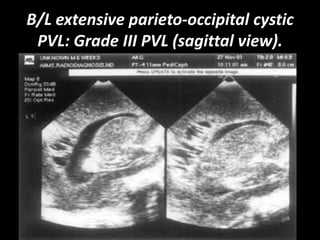
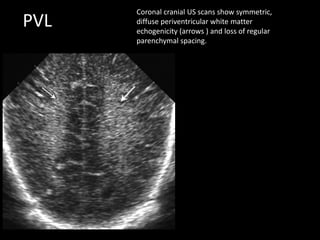
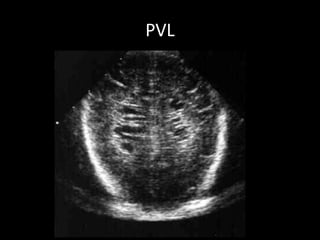
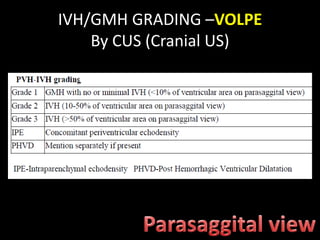
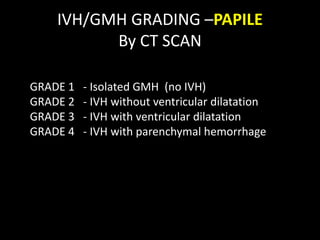
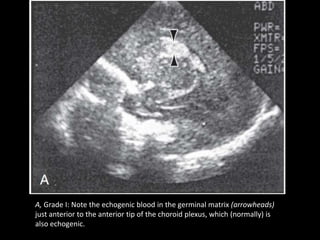
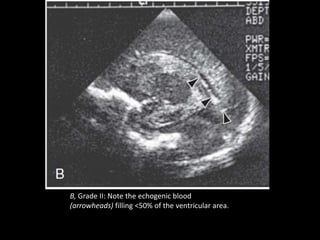




This document provides an overview of performing and interpreting a neurosonogram or cranial ultrasound. It describes the scanning planes and landmarks visualized. Key findings that can be identified include lateral ventricle size, cavum septum pellucidum, corpus callosum, brainstem, and choroid plexus. Grading scales are provided for periventricular leukomalacia and intraventricular hemorrhage. Doppler measurements of blood flow velocities are also described. The document serves as a guide for systematically scanning the brain and identifying both normal anatomy and common abnormalities on cranial ultrasound in neonates and infants.




































![NSG AND HIE [Autosaved].............pptx](https://cdn.slidesharecdn.com/ss_thumbnails/nsgandhieautosaved-250908133023-52fc5444-thumbnail.jpg?width=640&height=640&fit=bounds)

























































