Downloaded 692 times
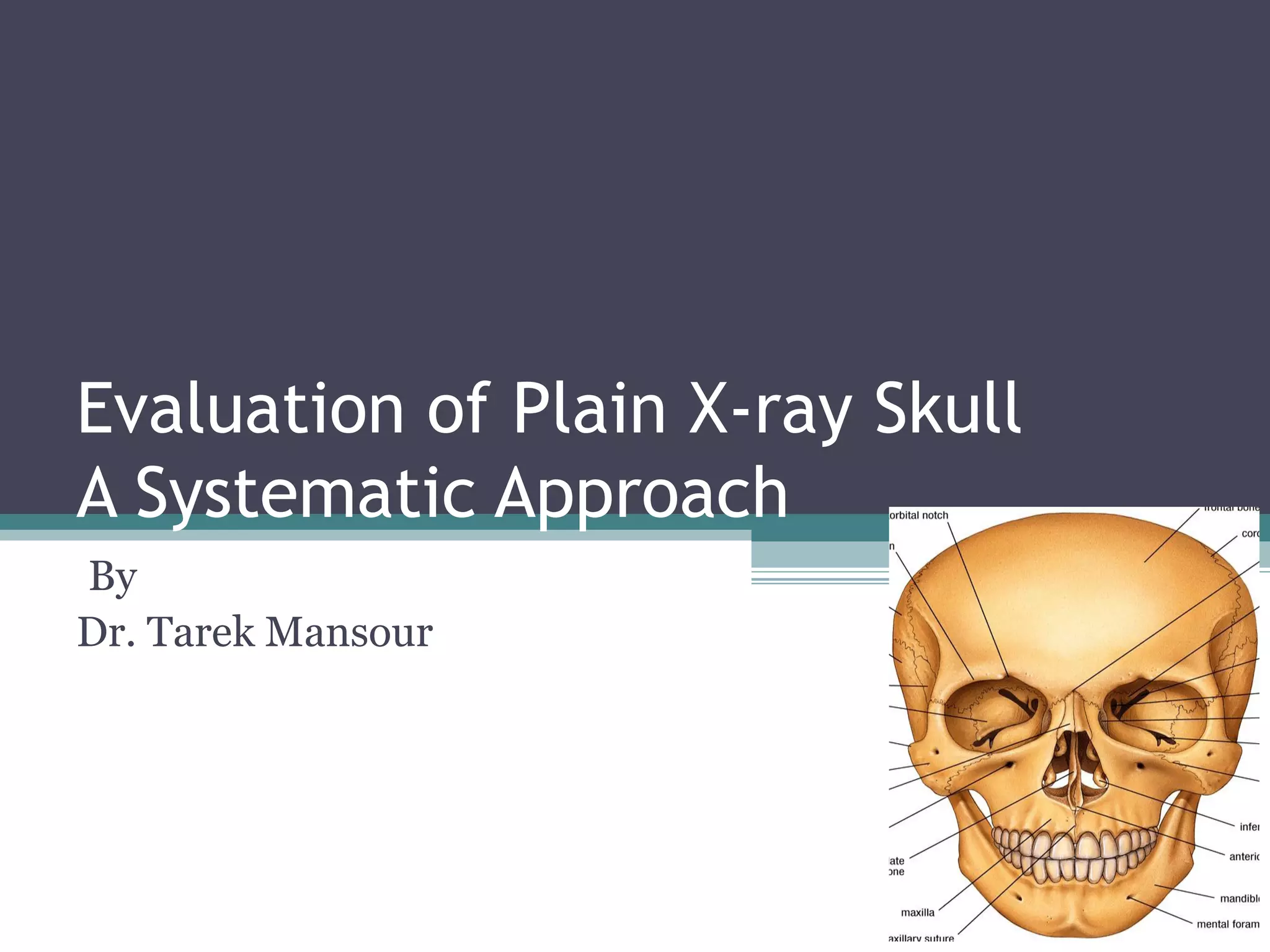
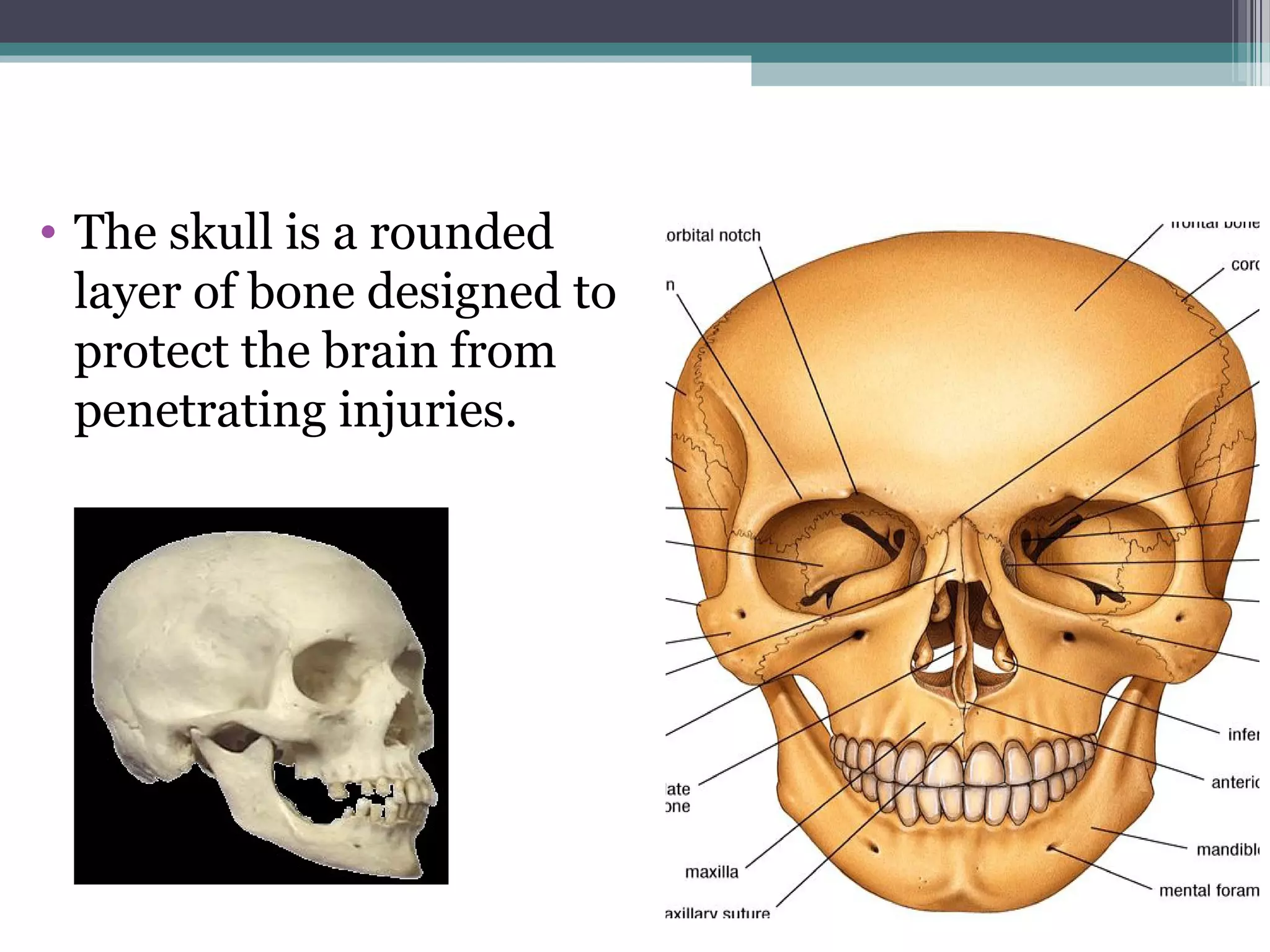
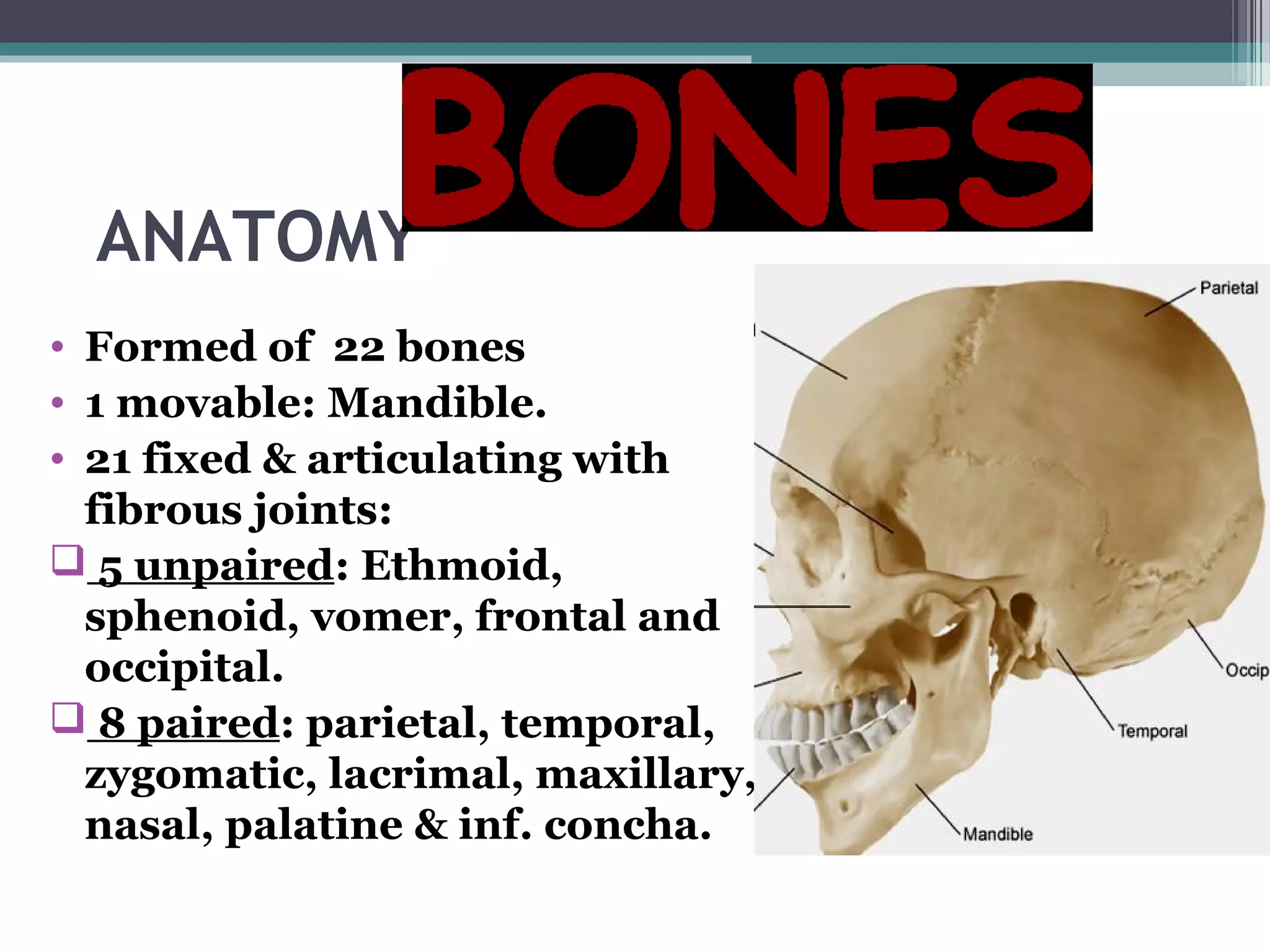
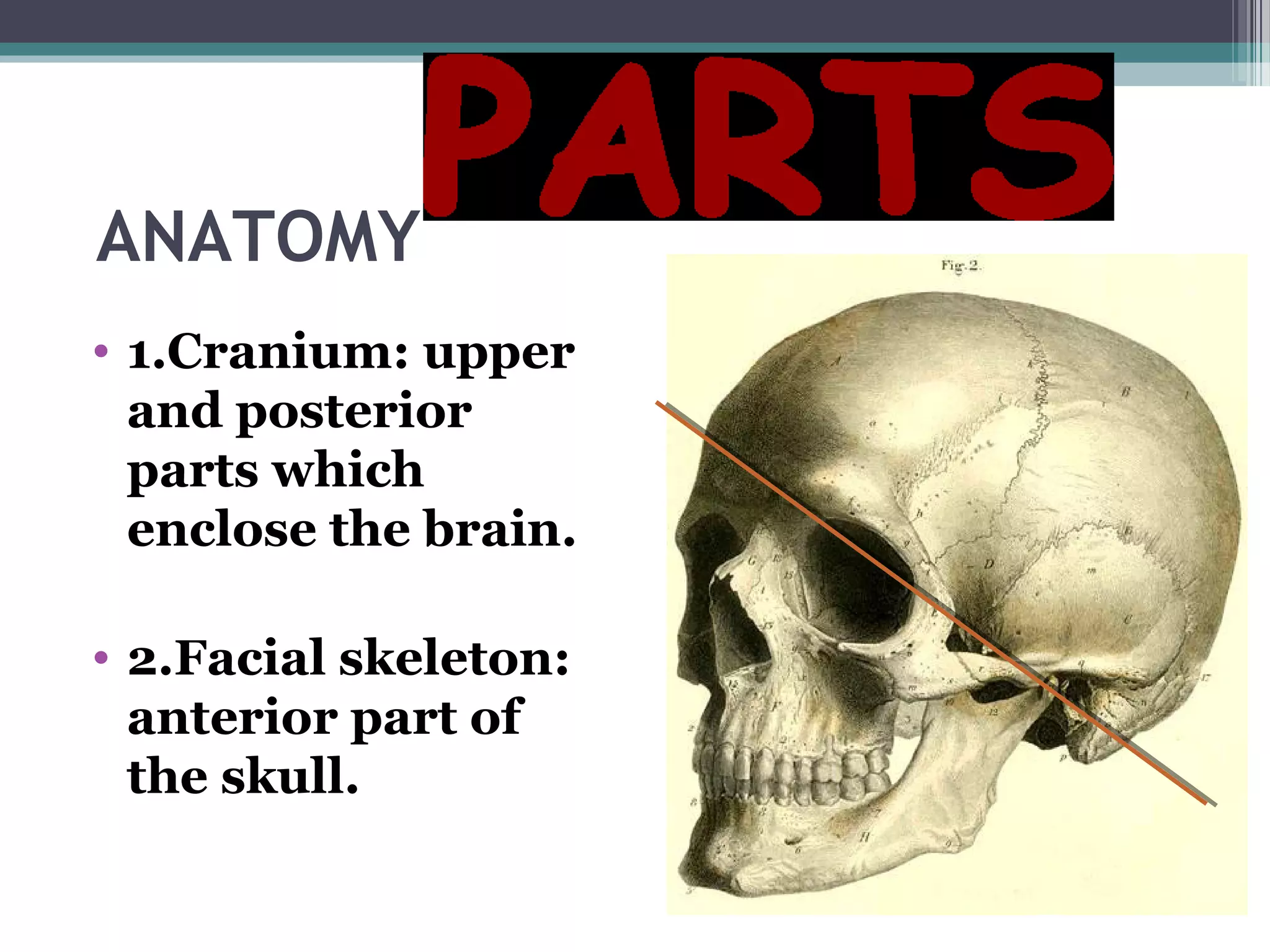
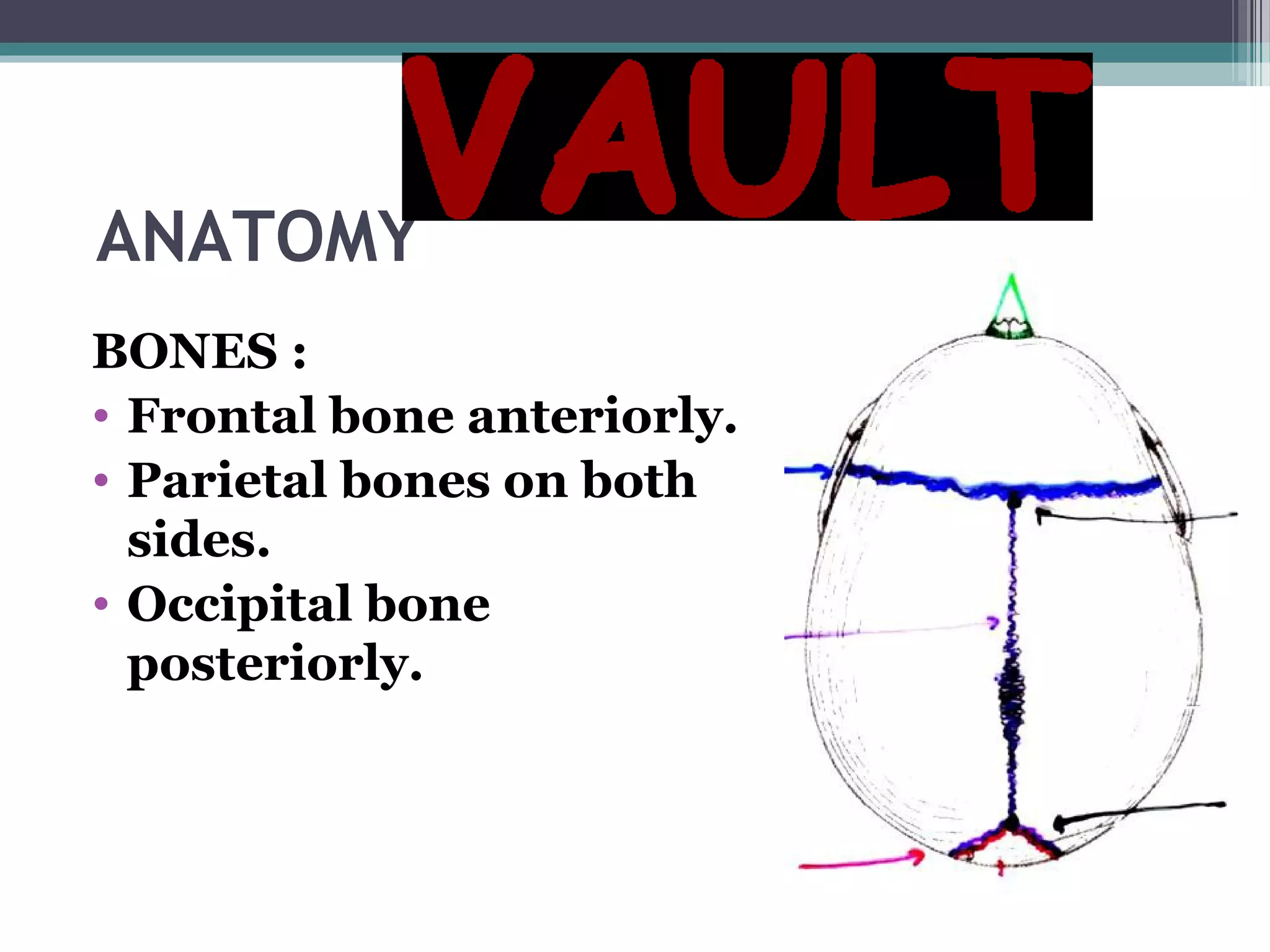
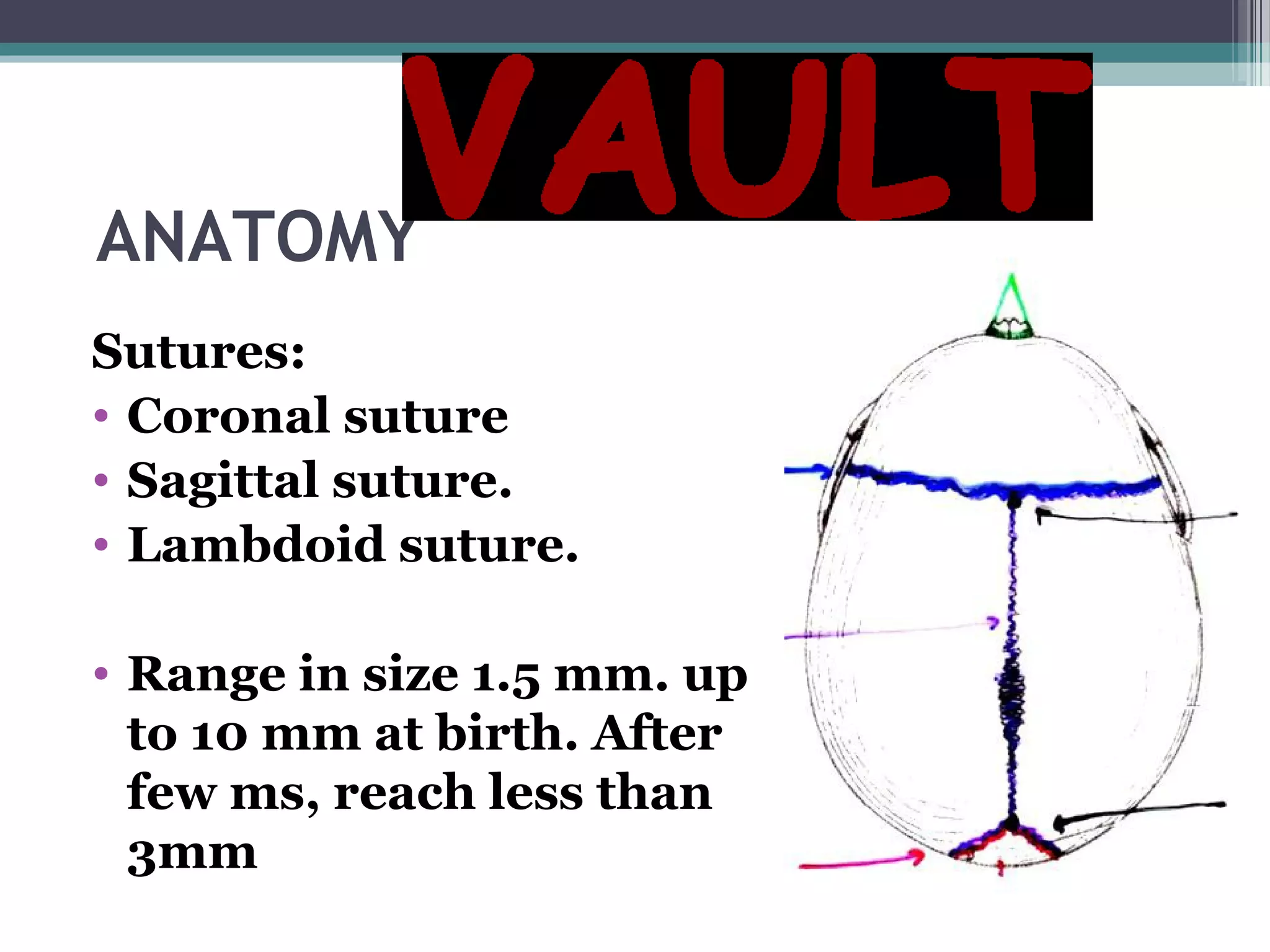
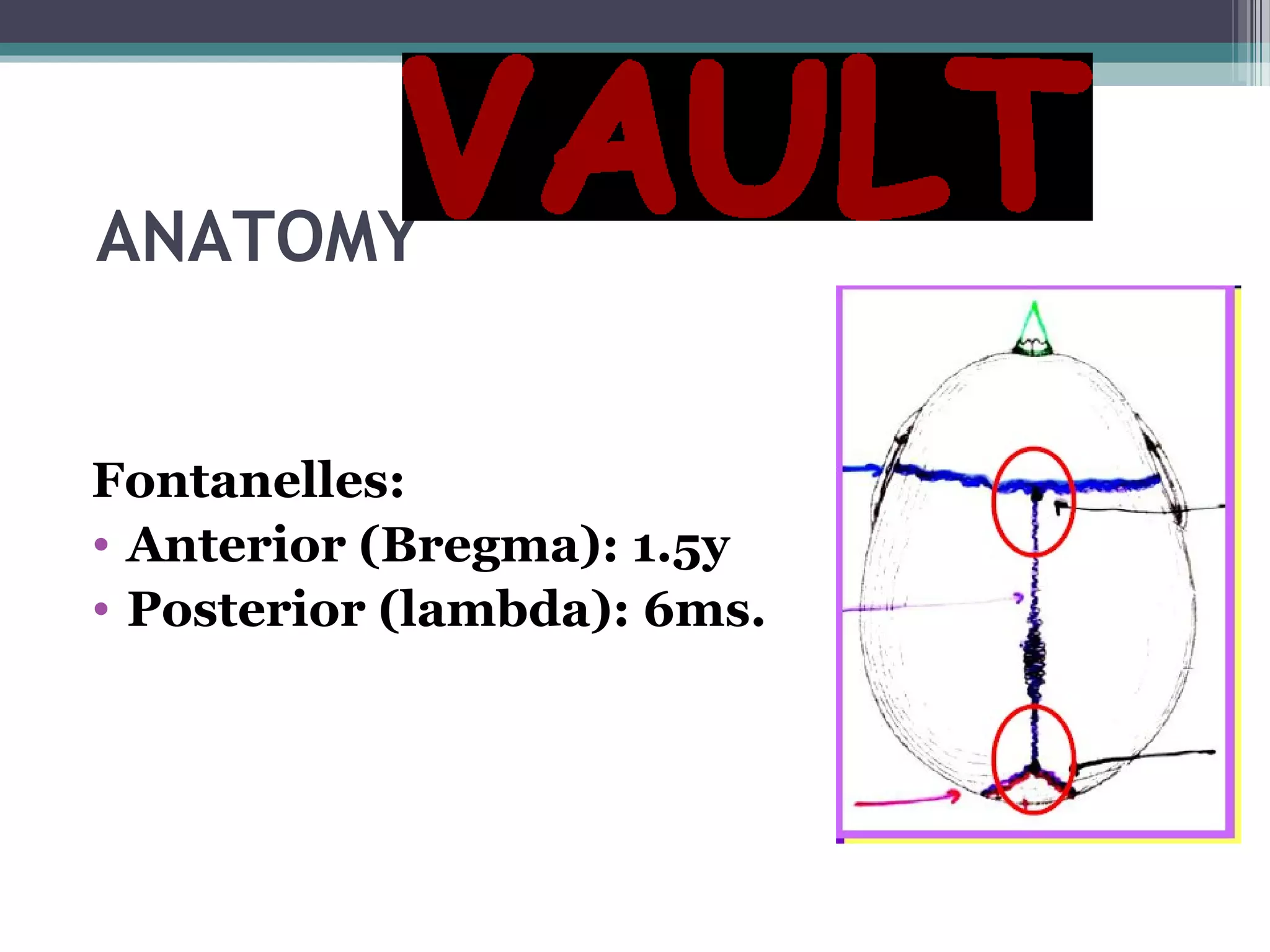
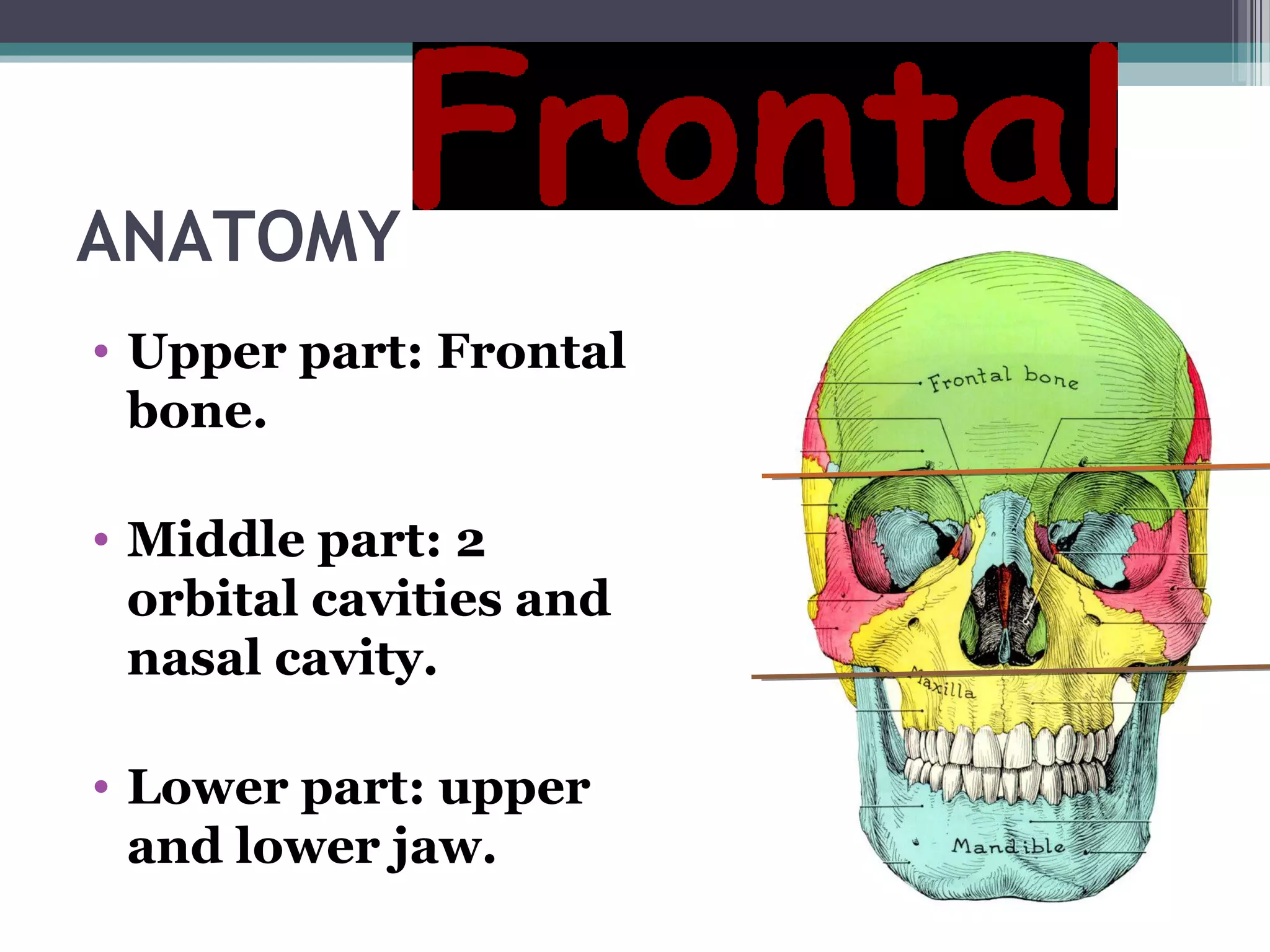
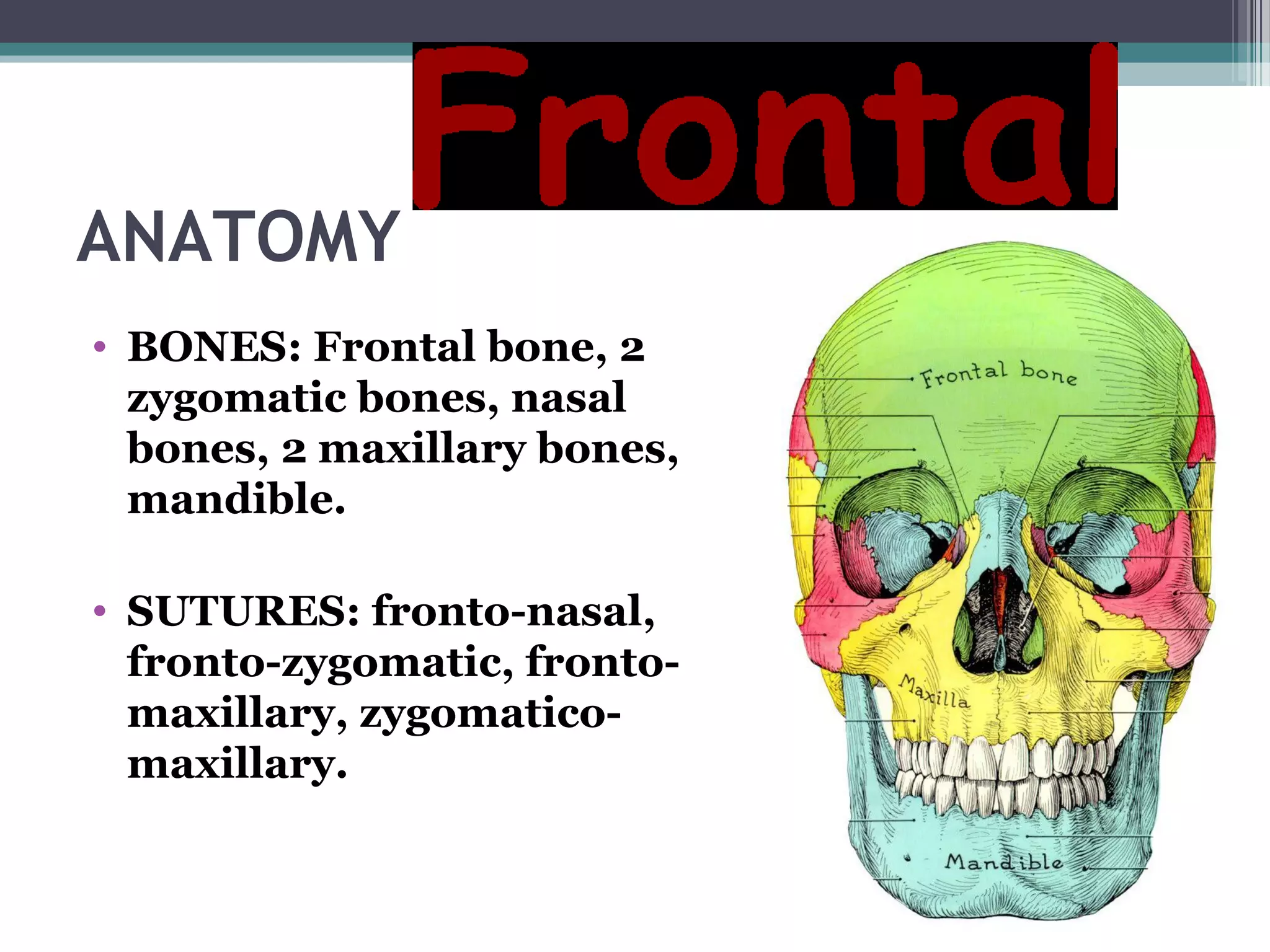
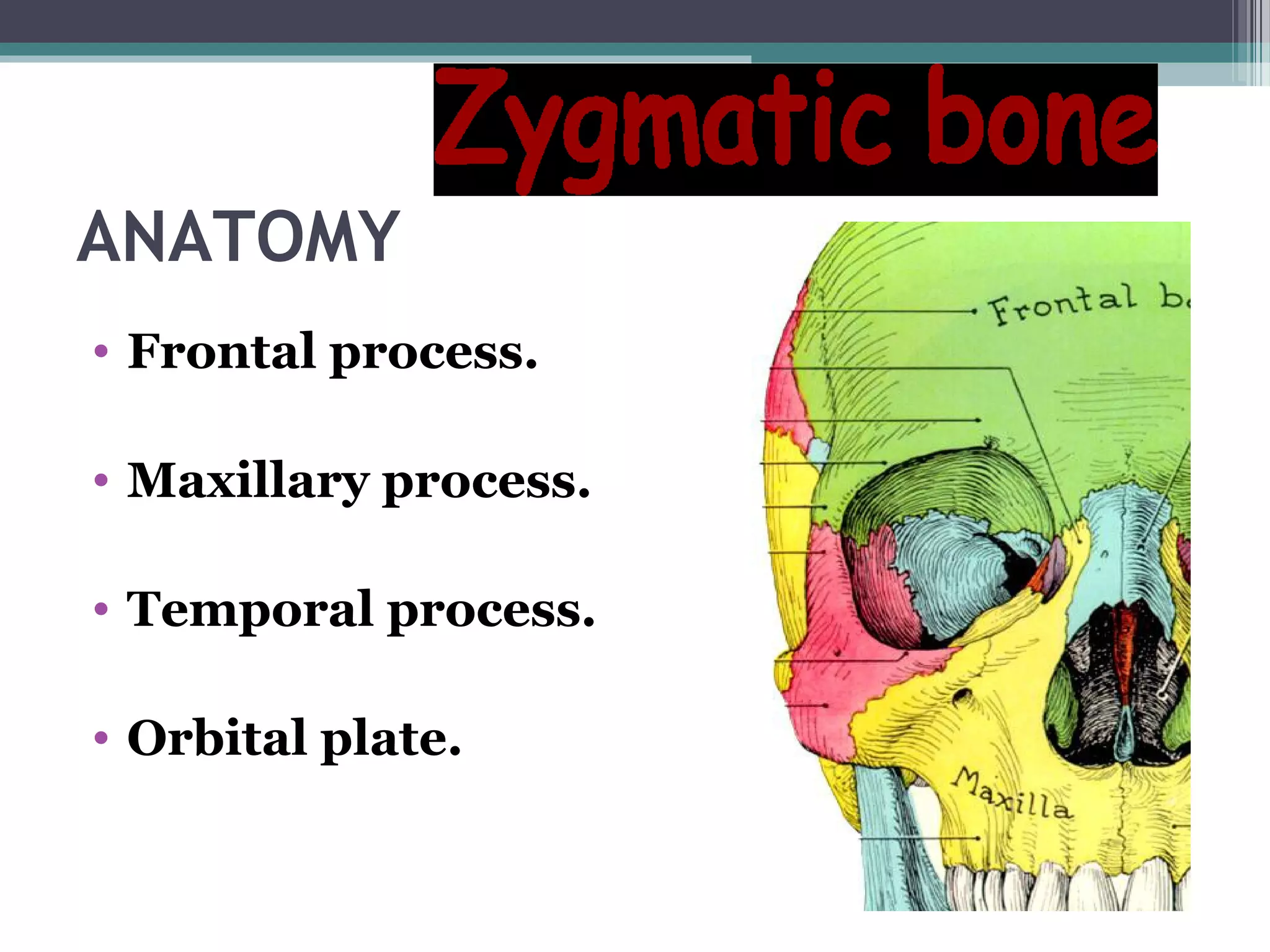
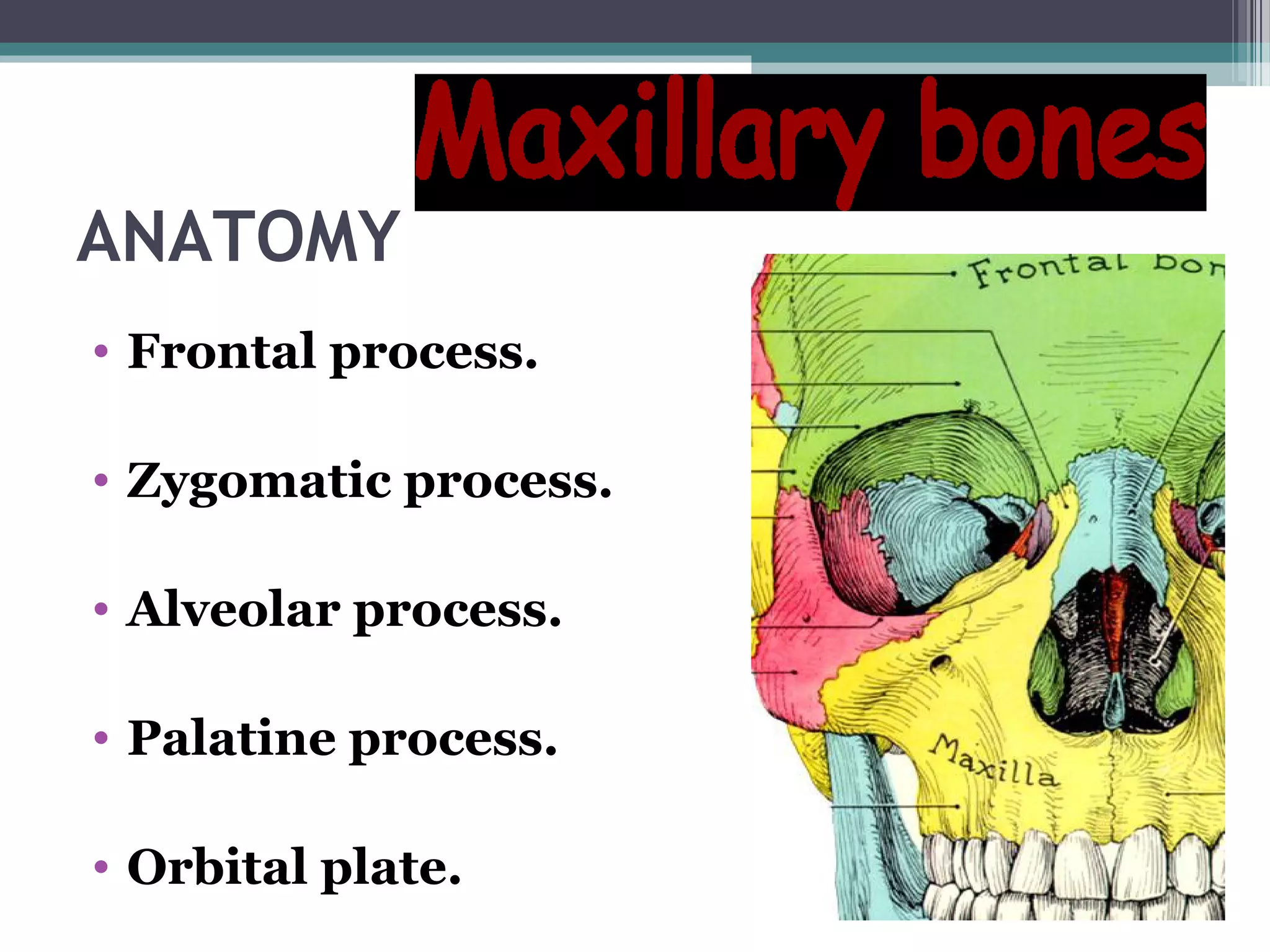
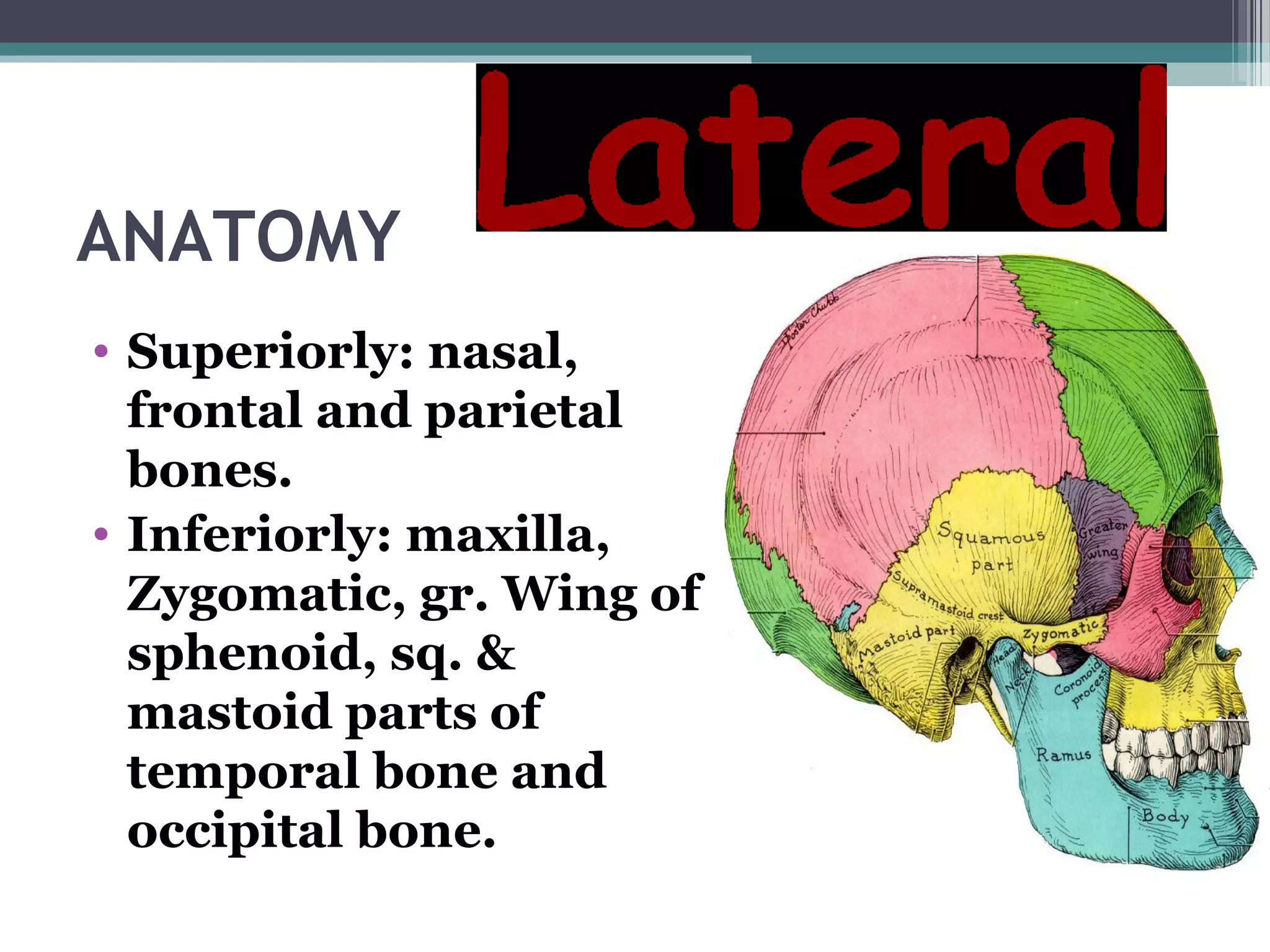
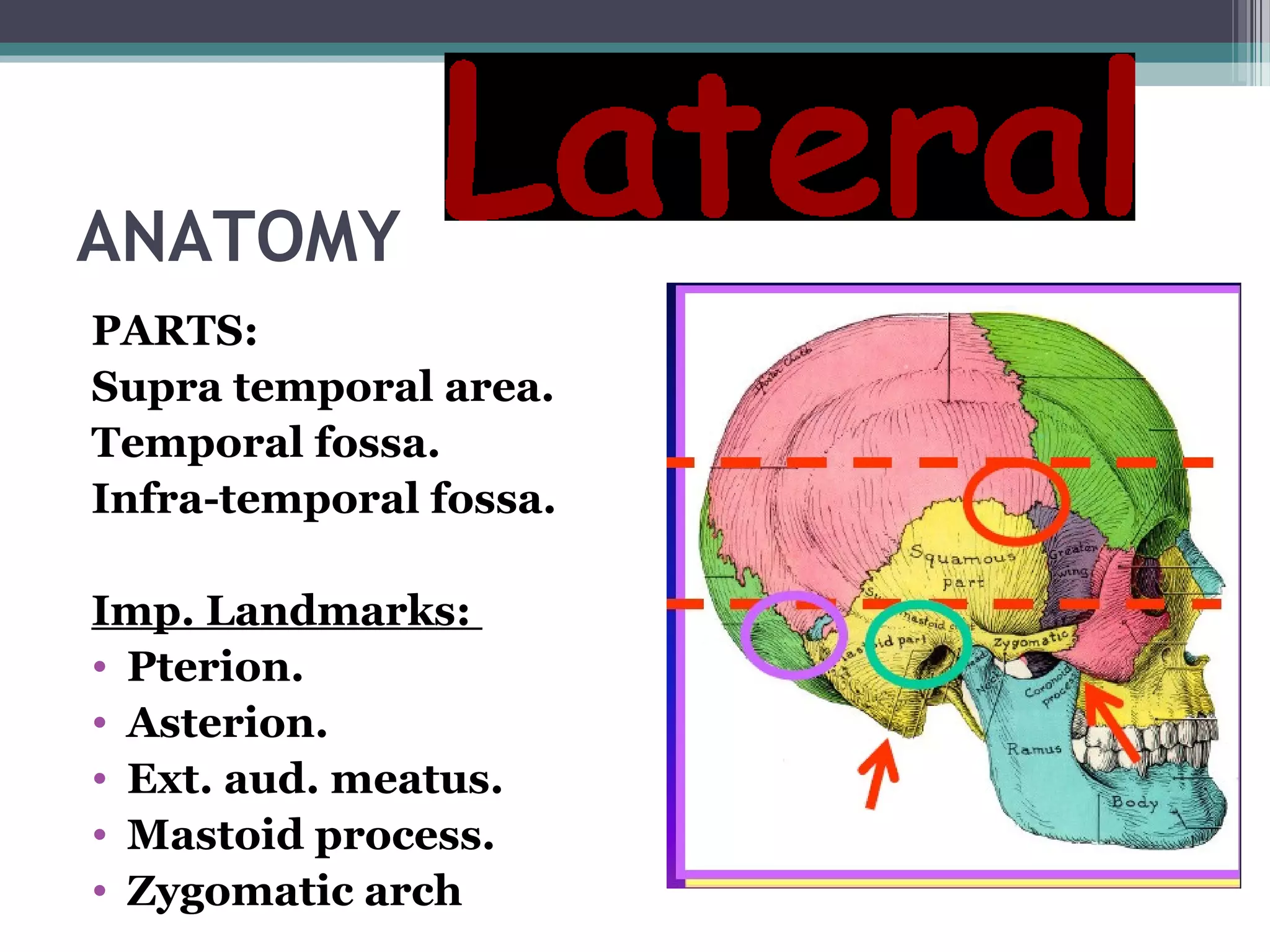
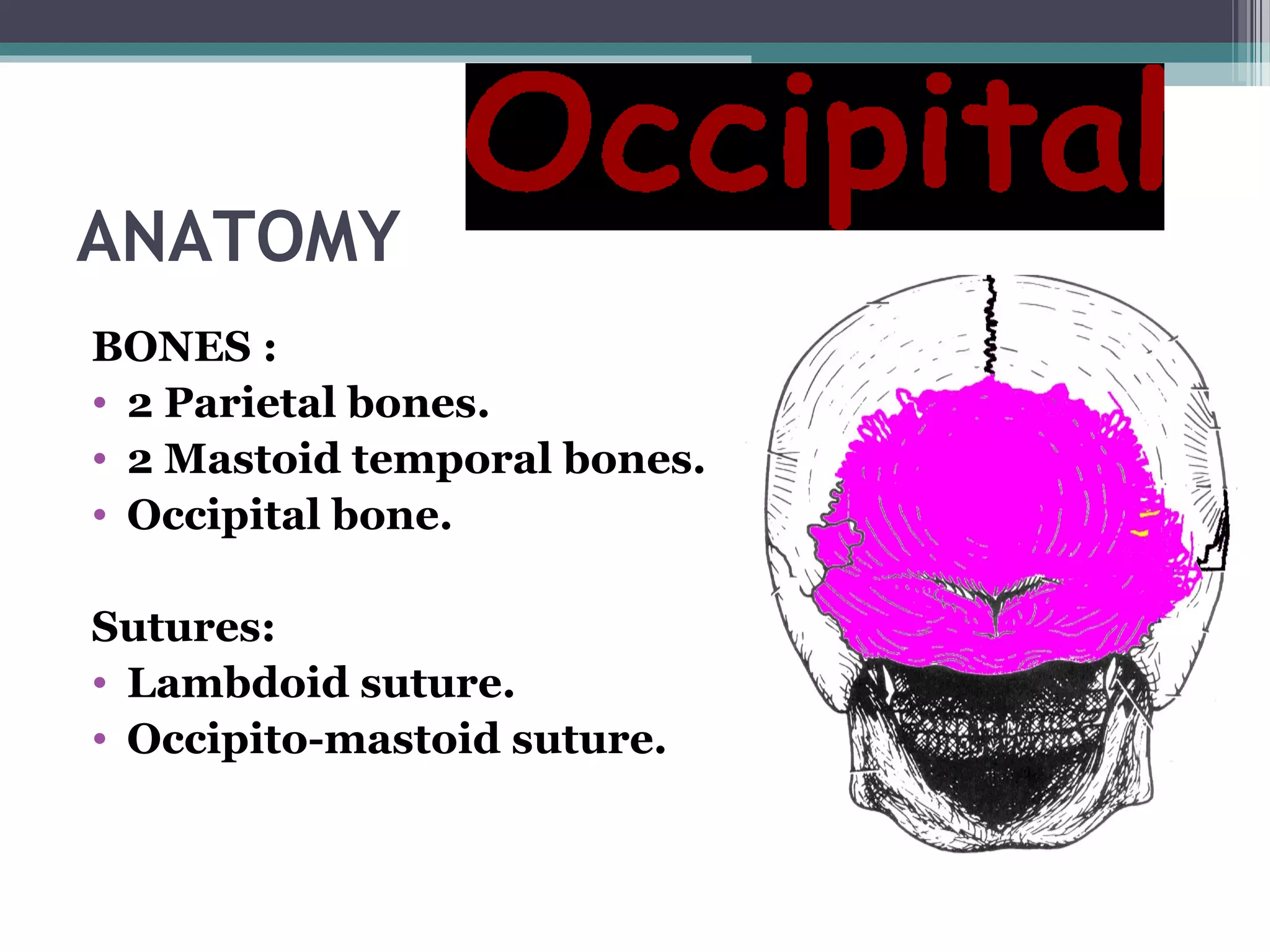
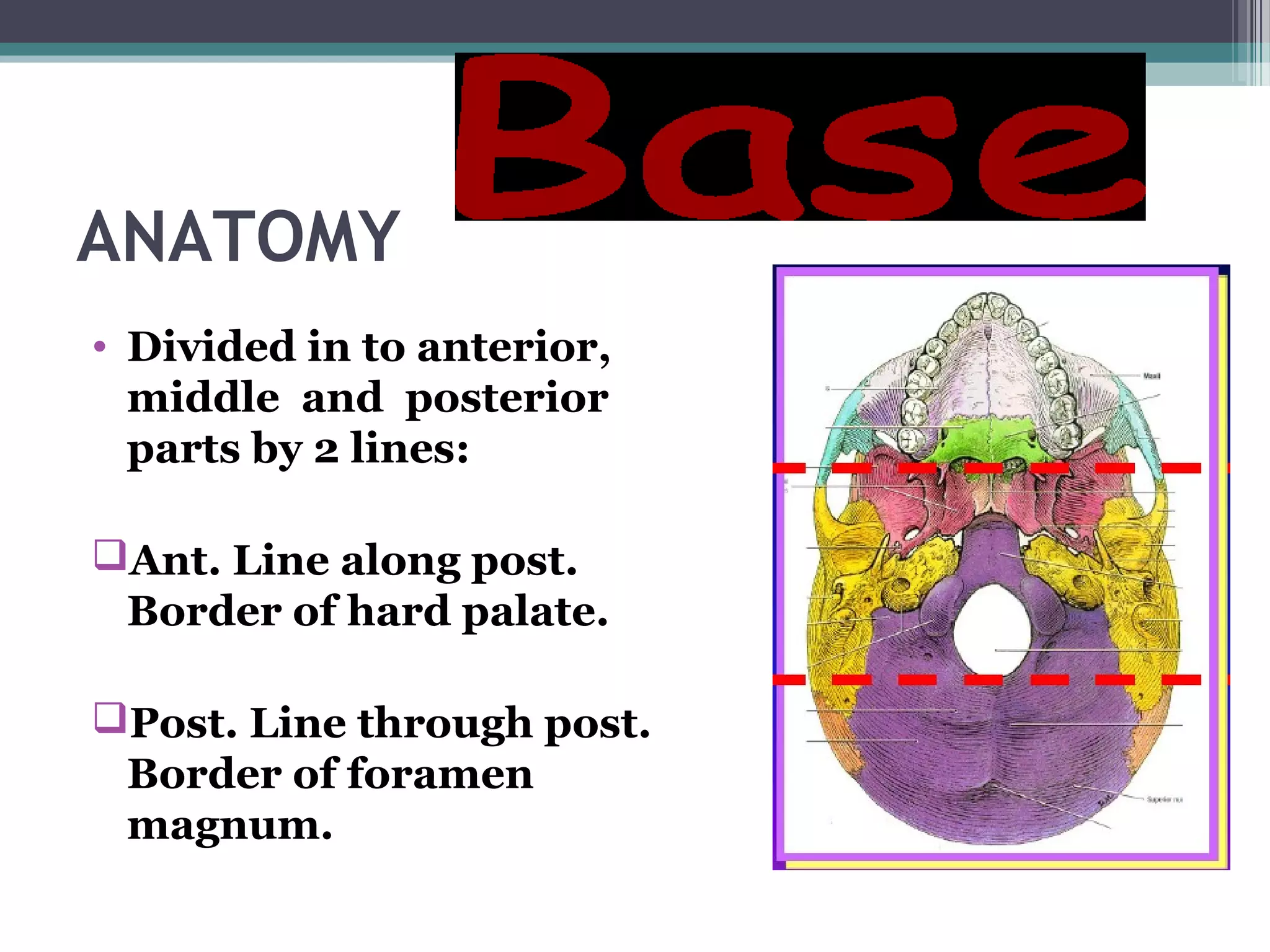
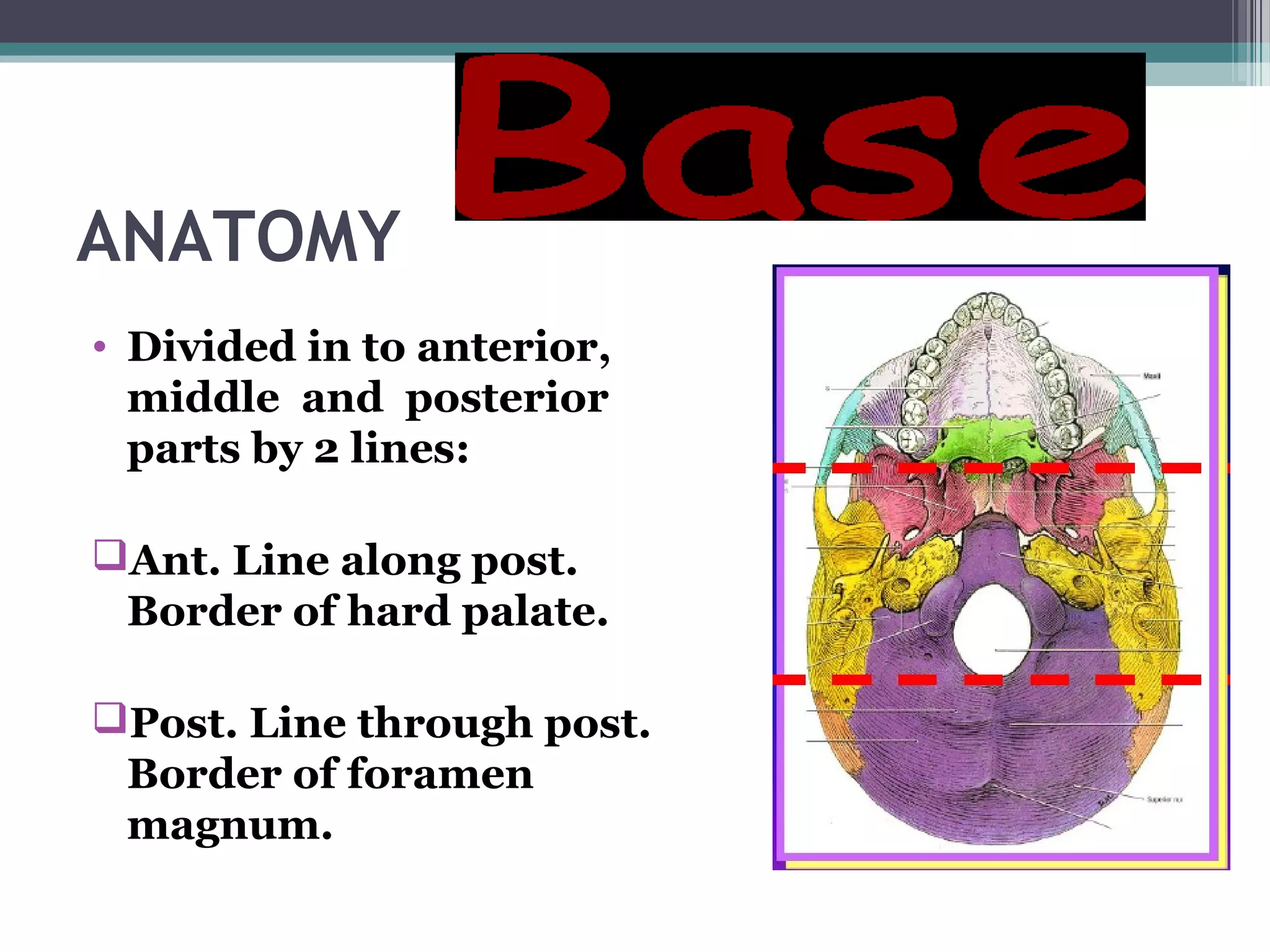
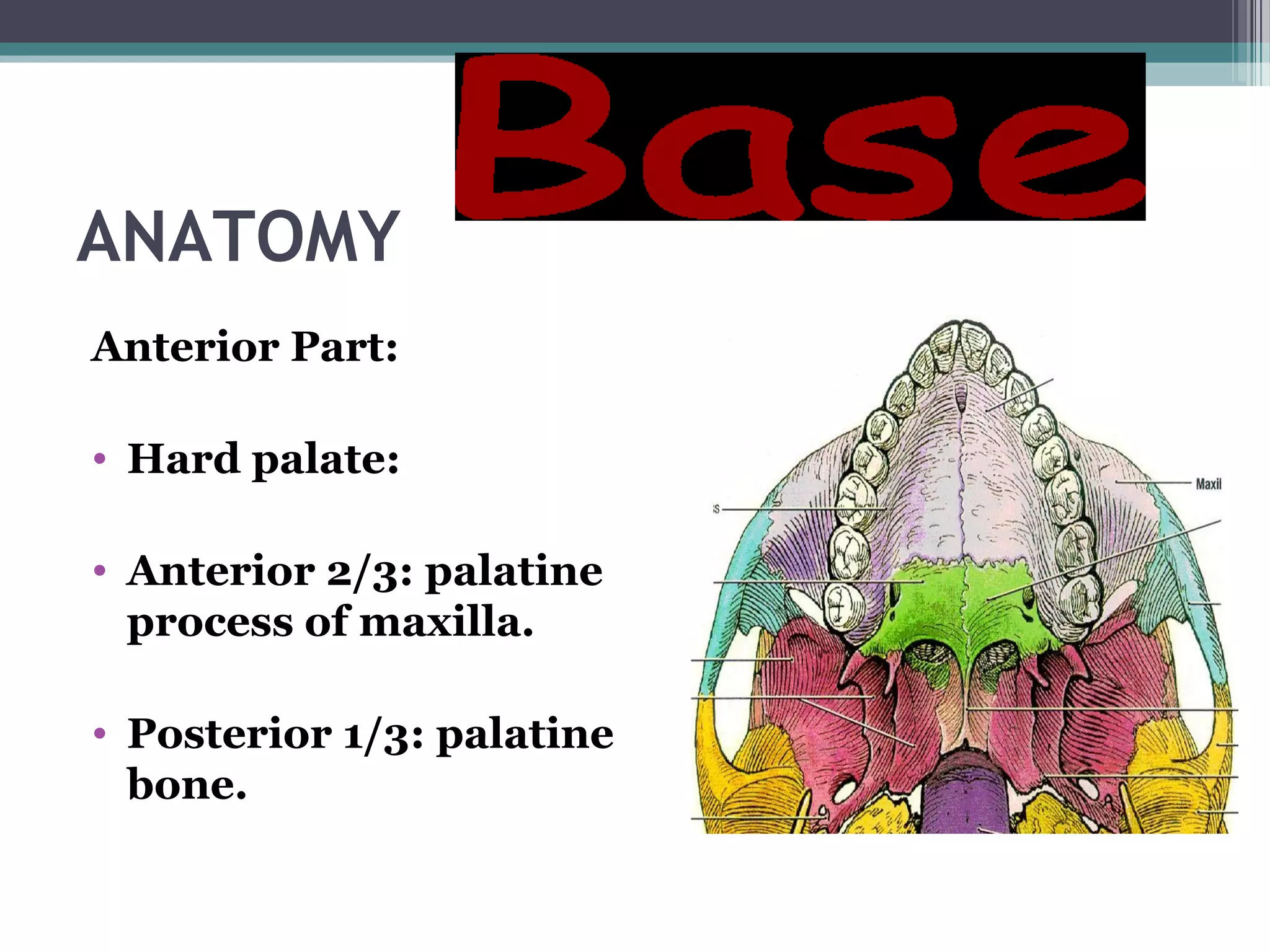
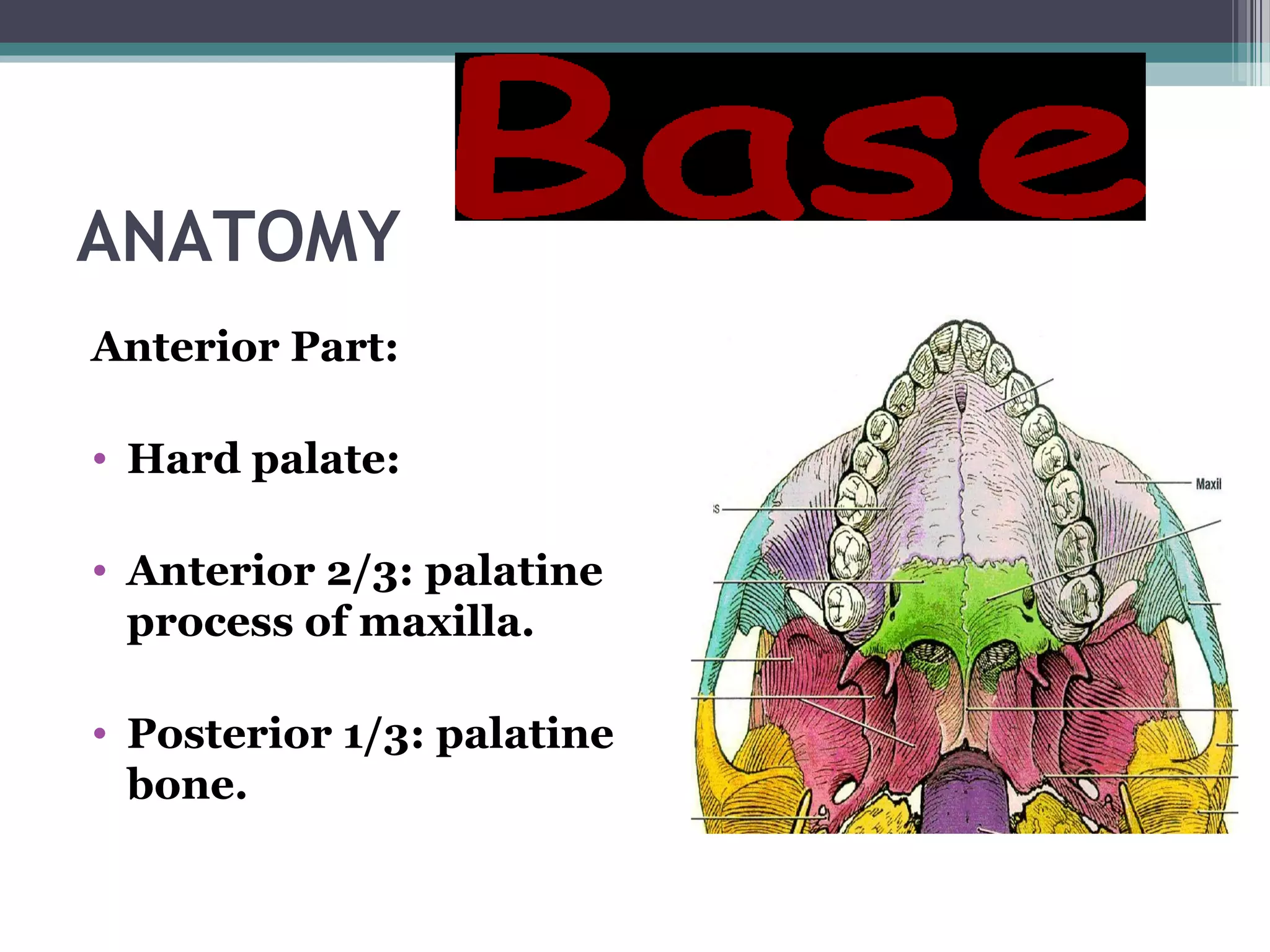
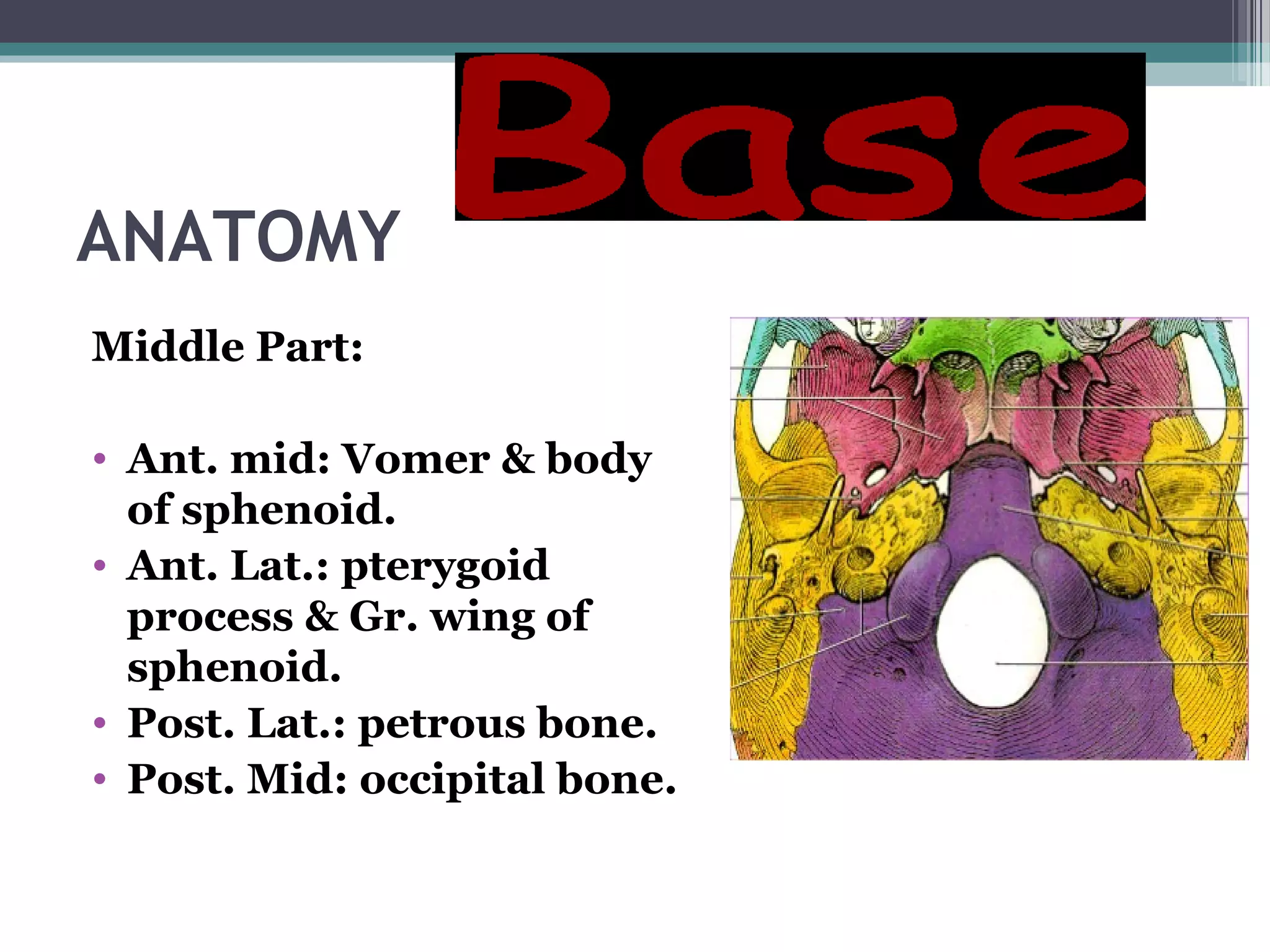
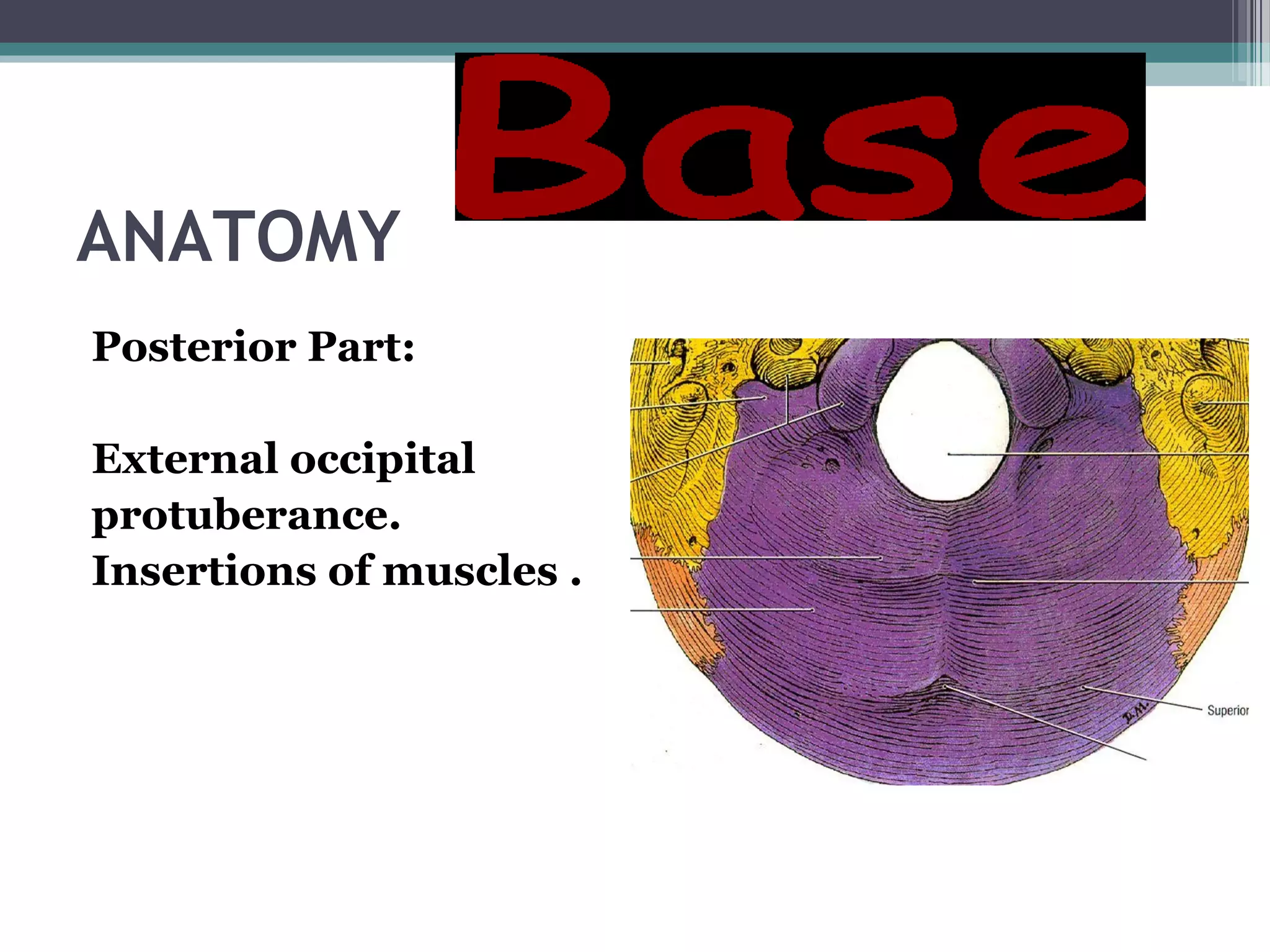
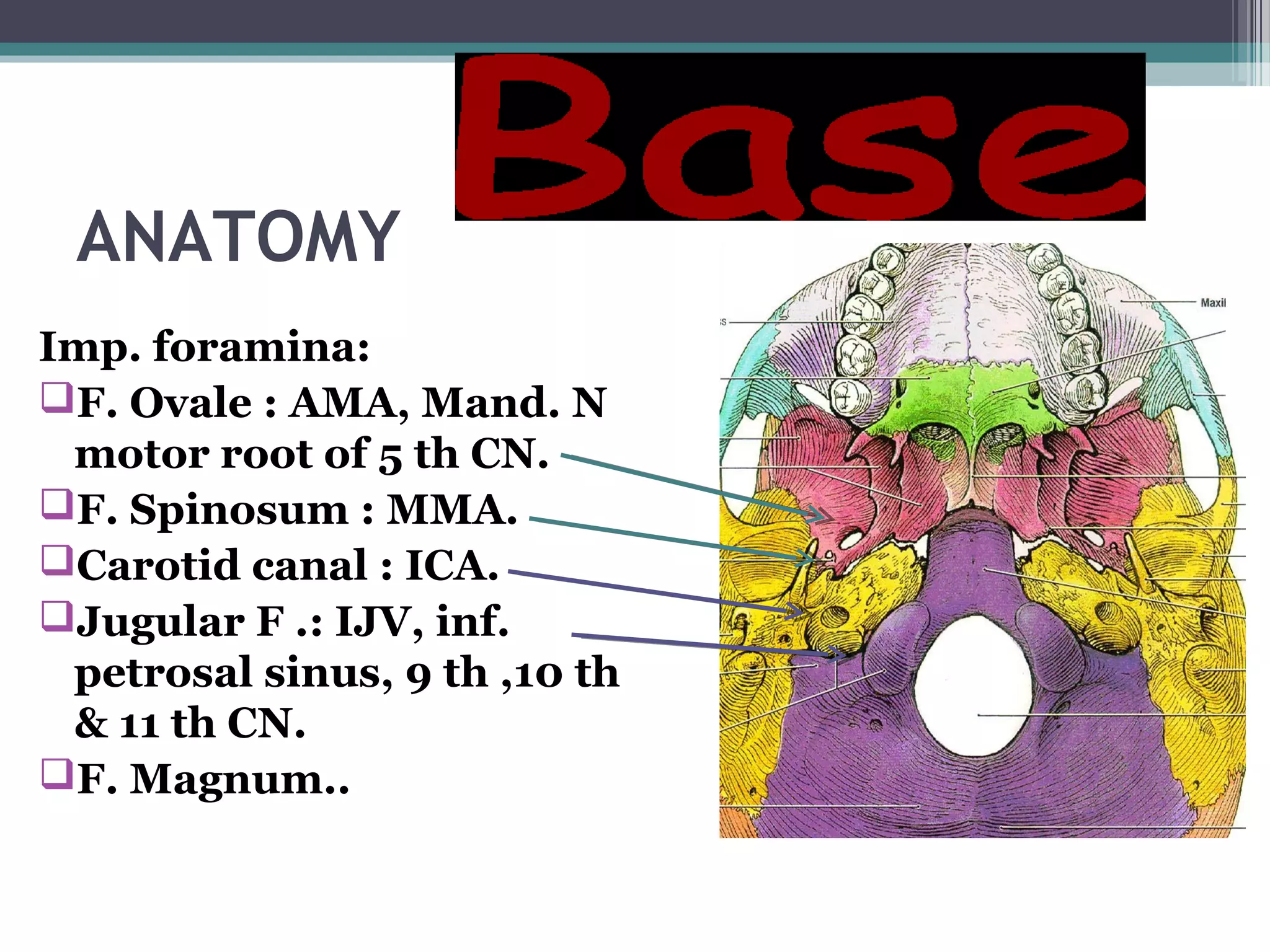
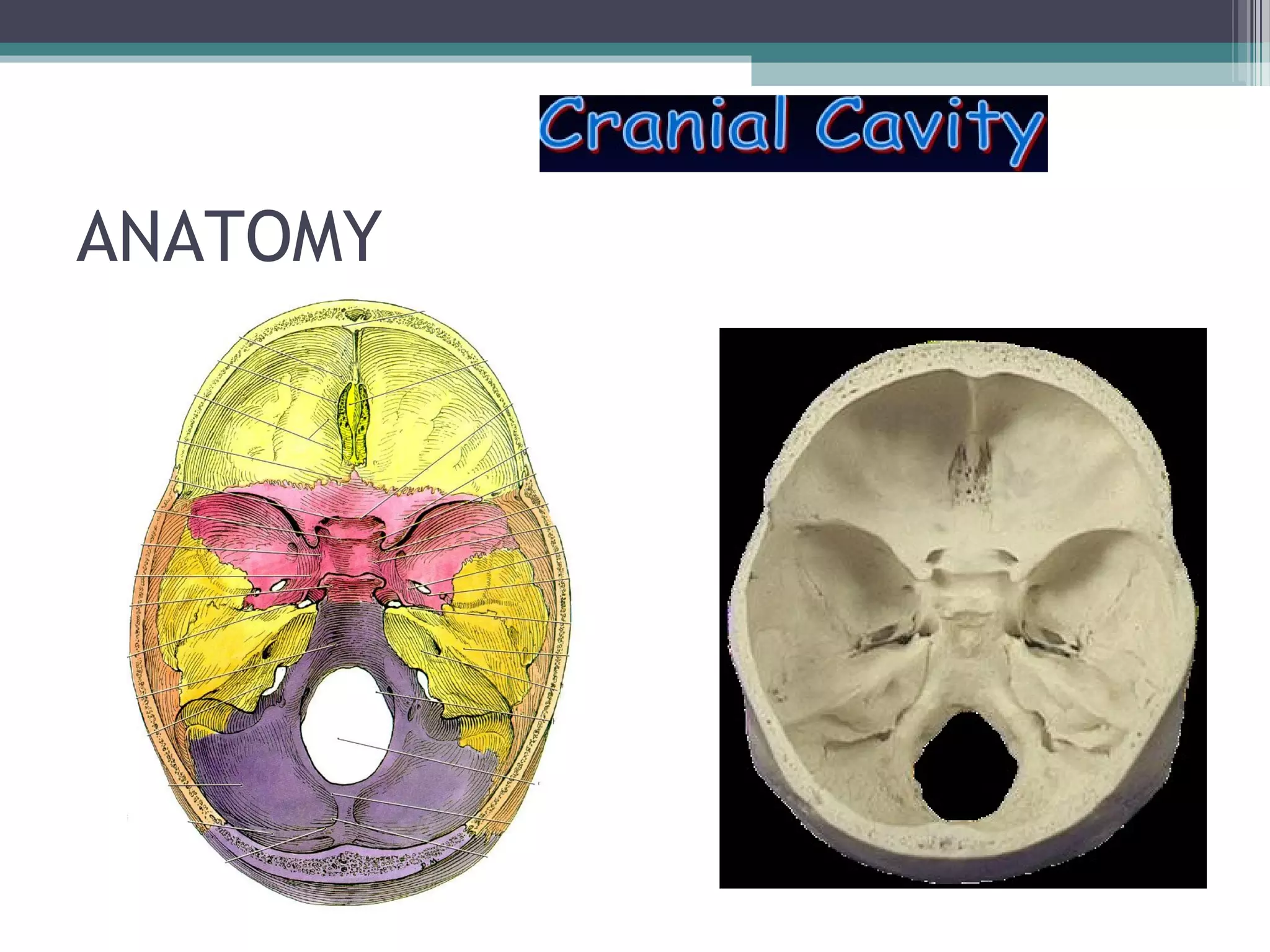
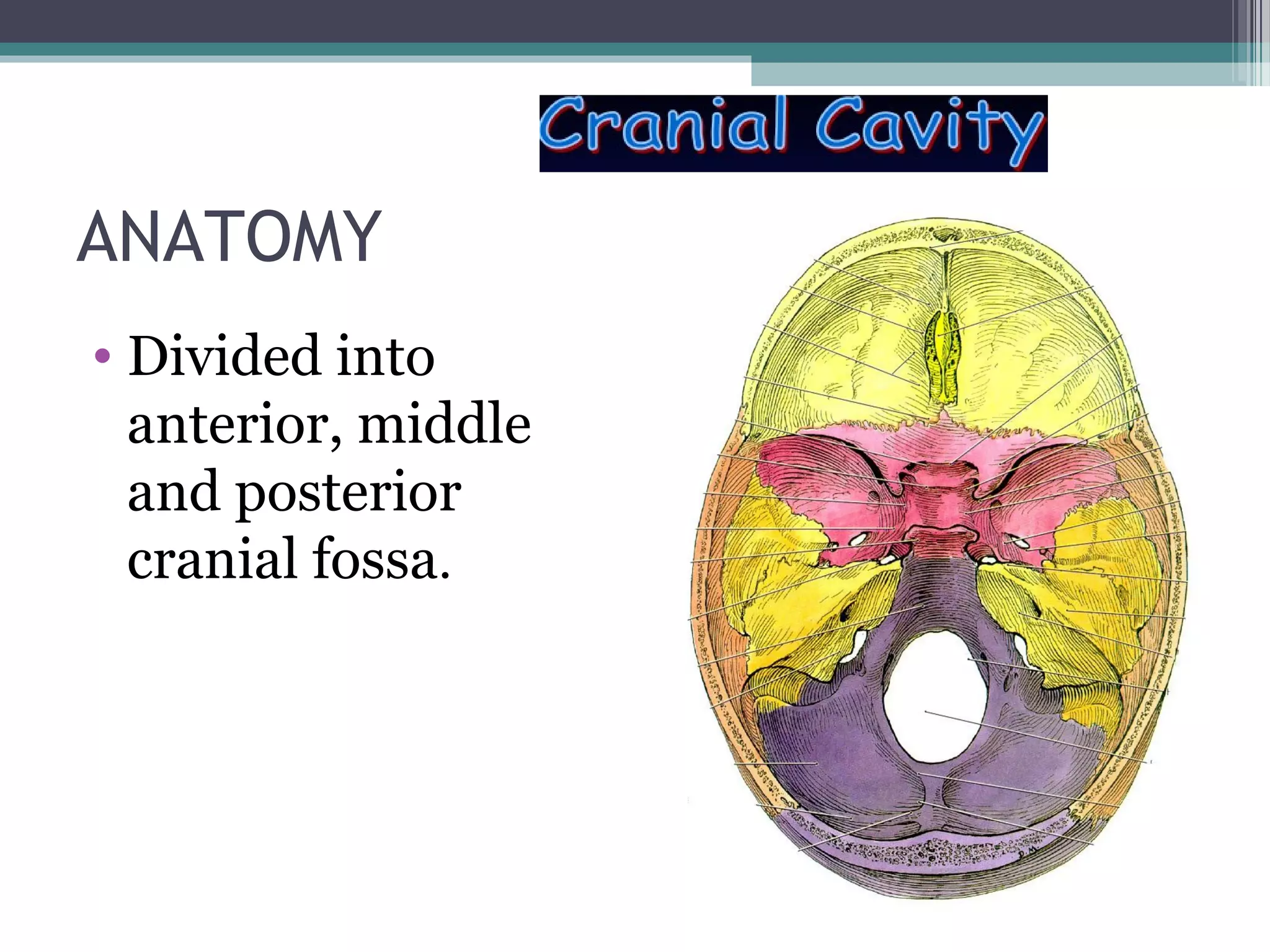
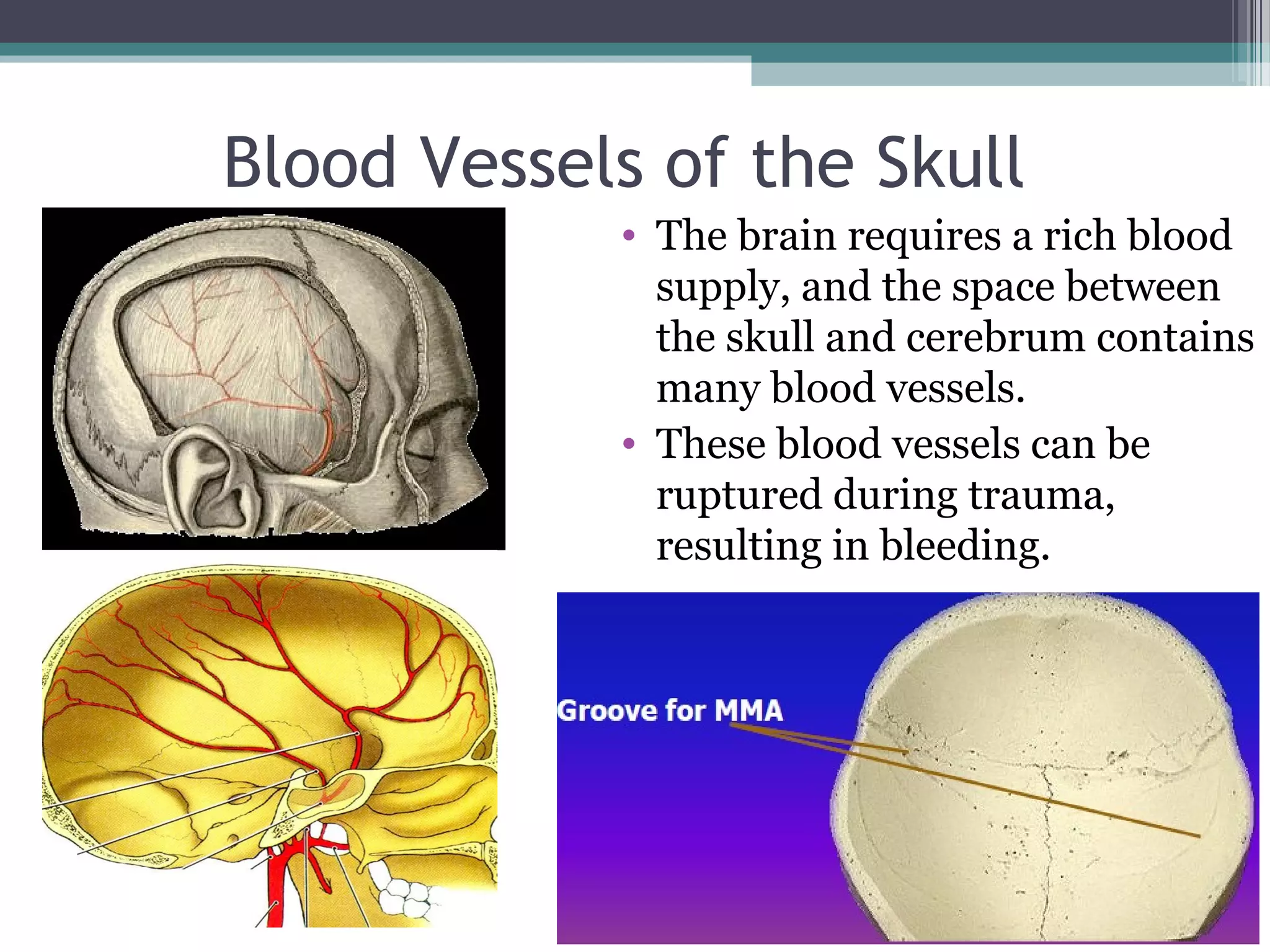
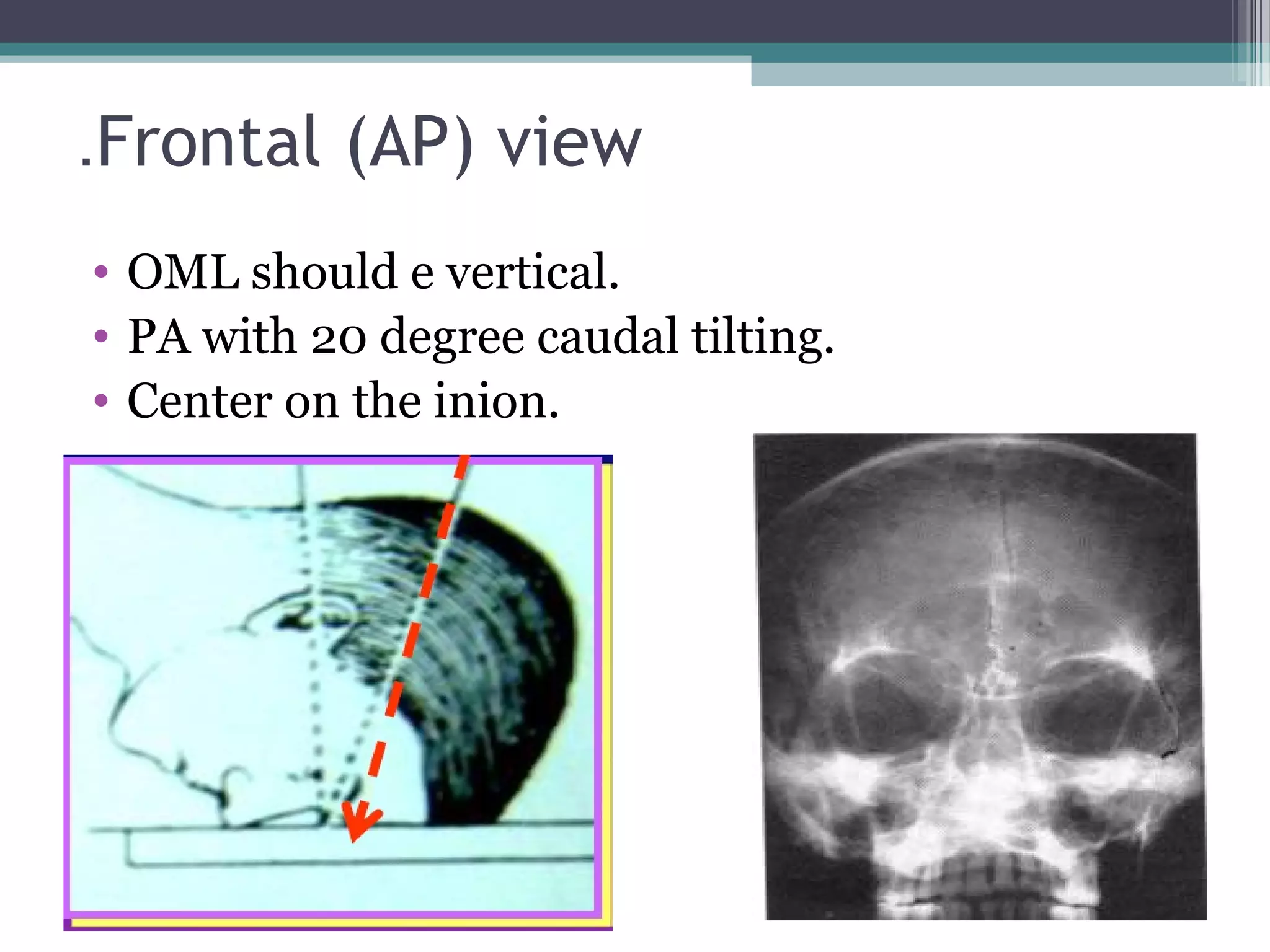
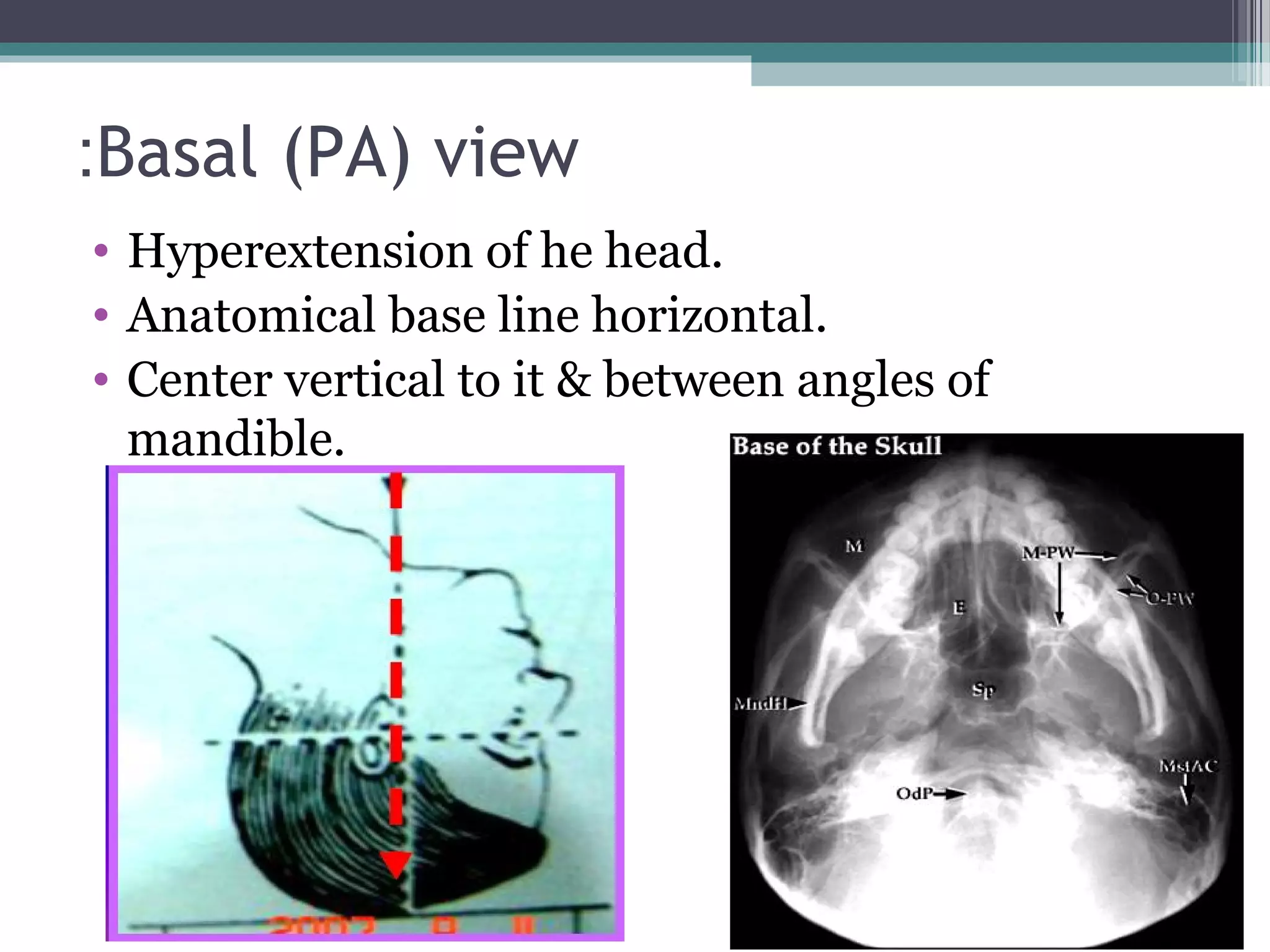
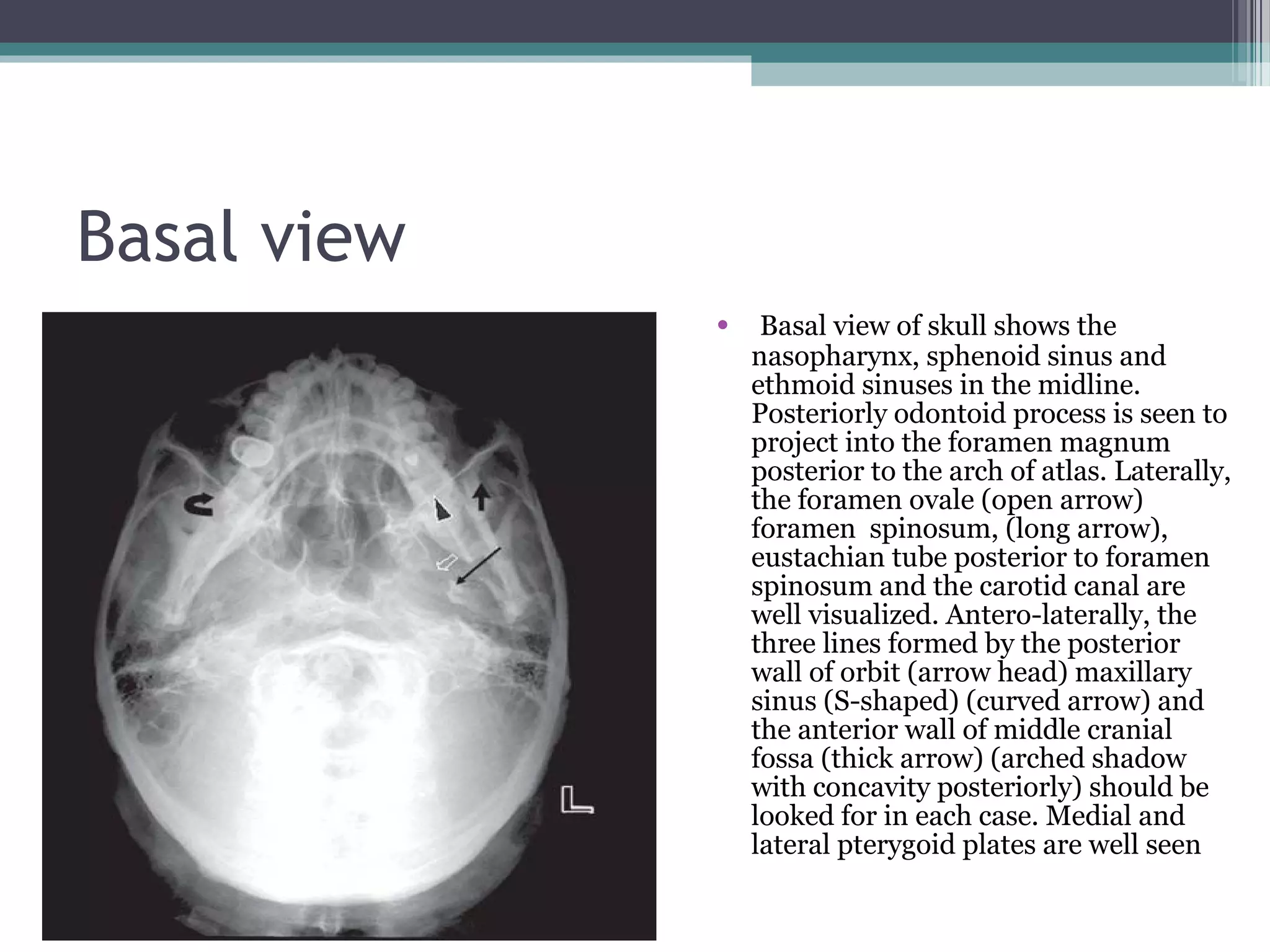
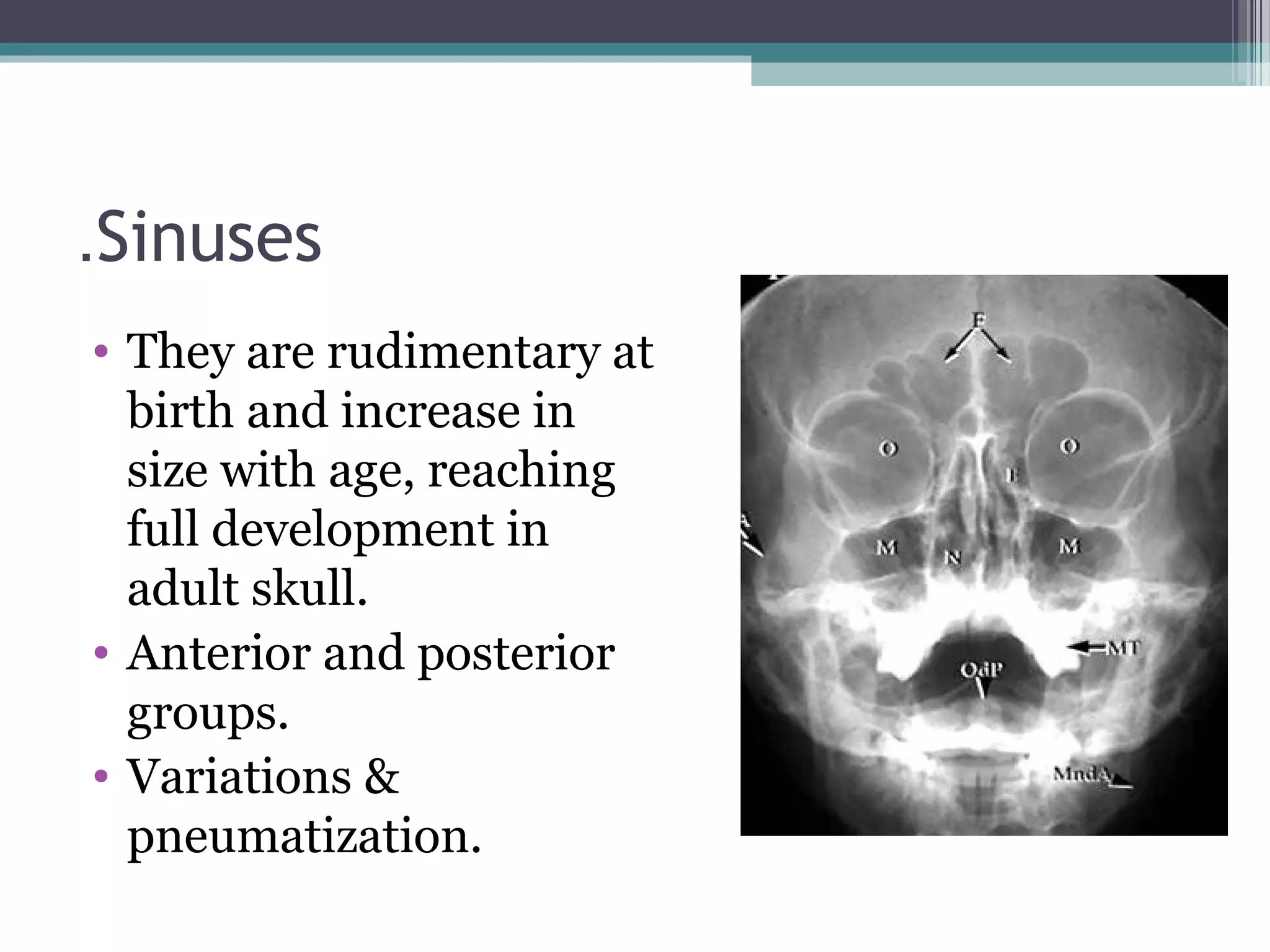
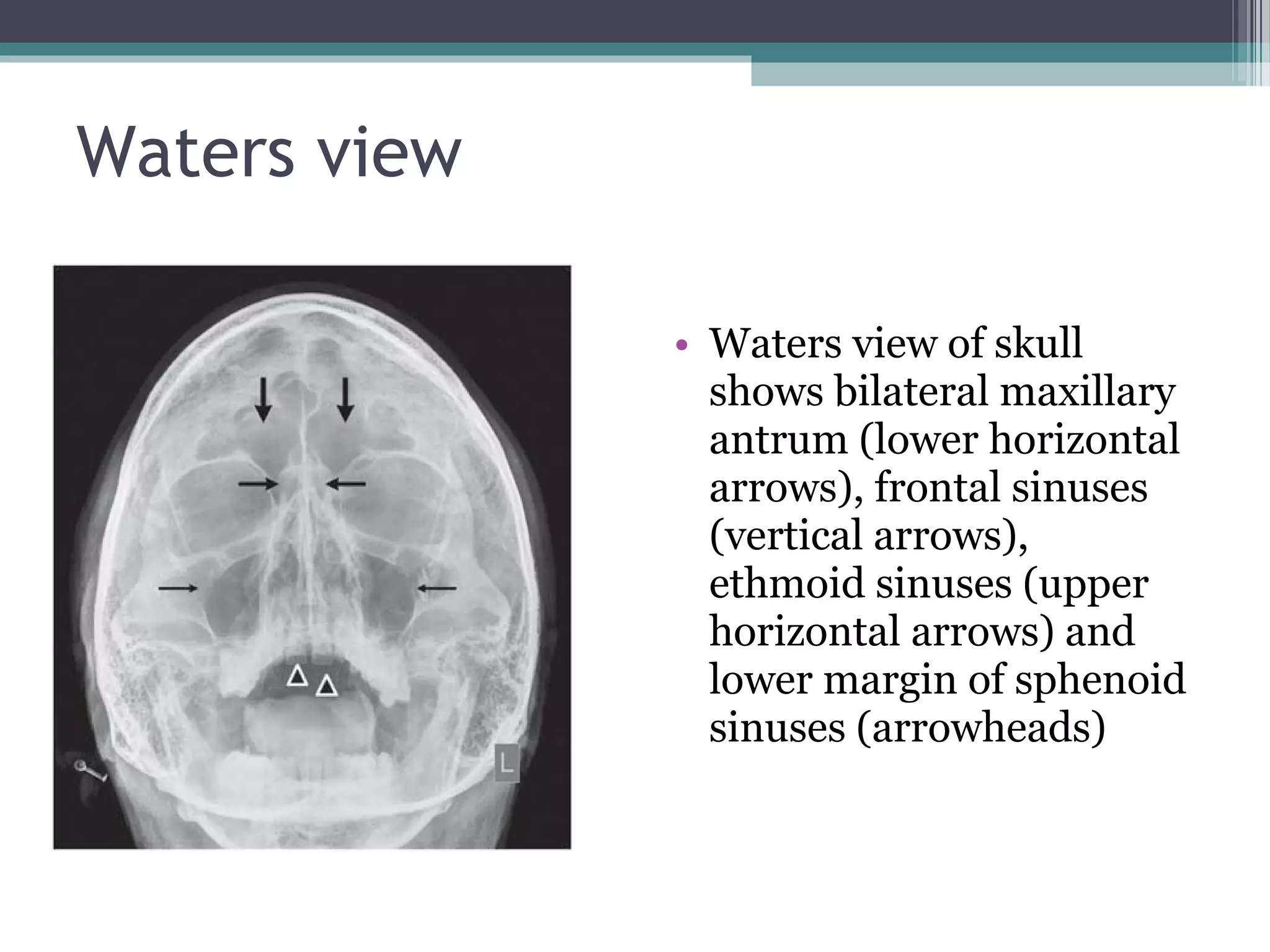
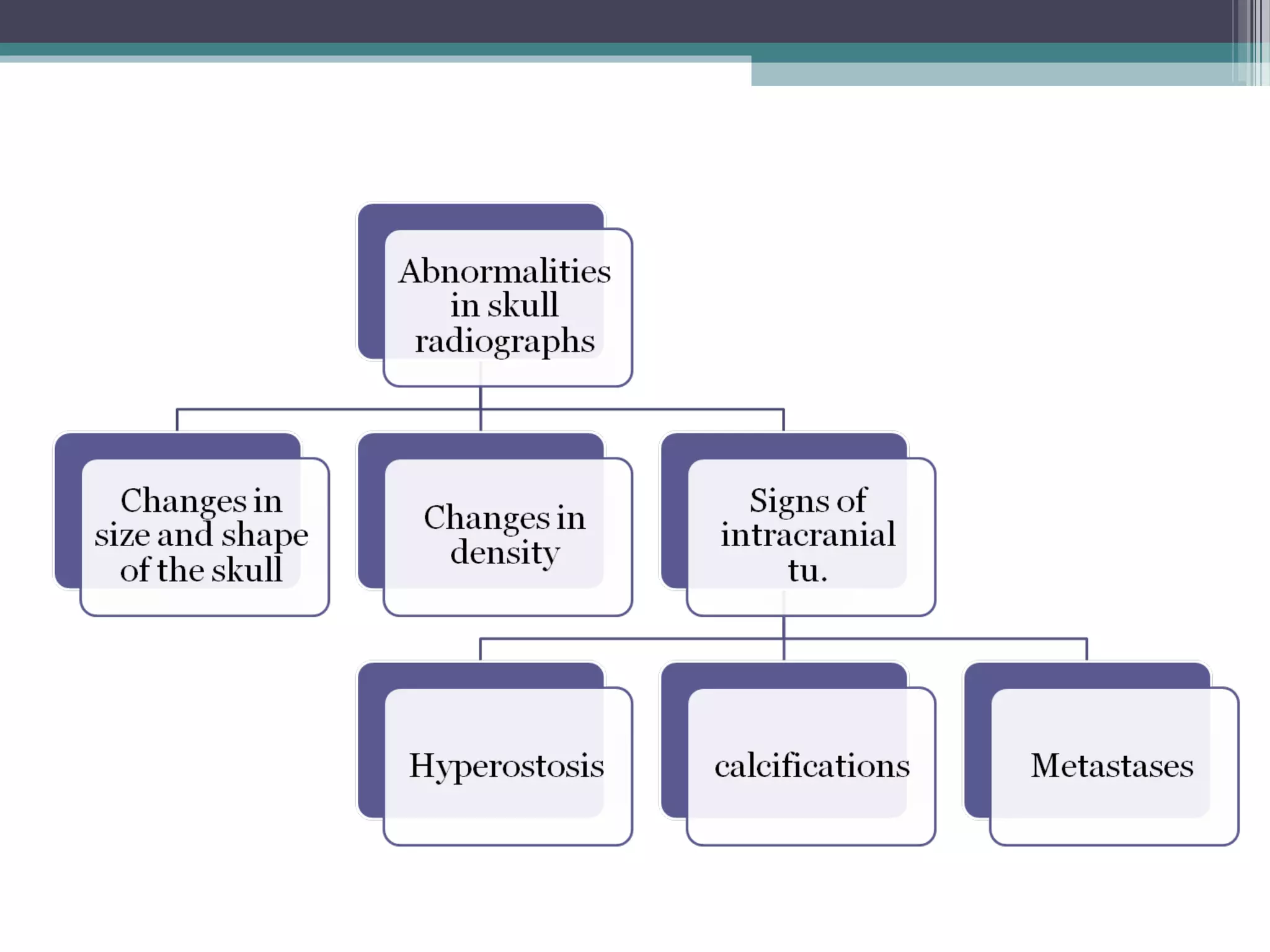
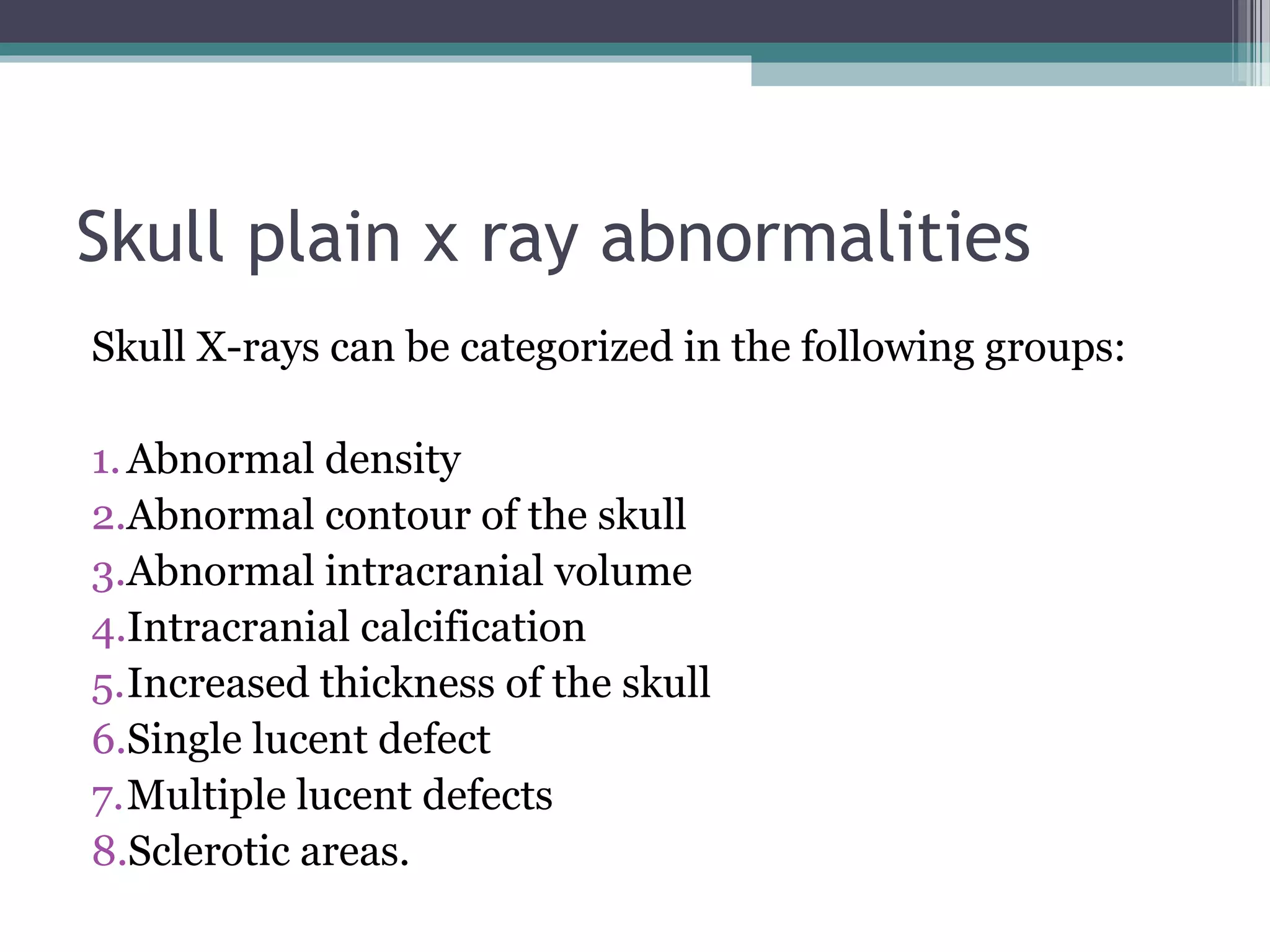
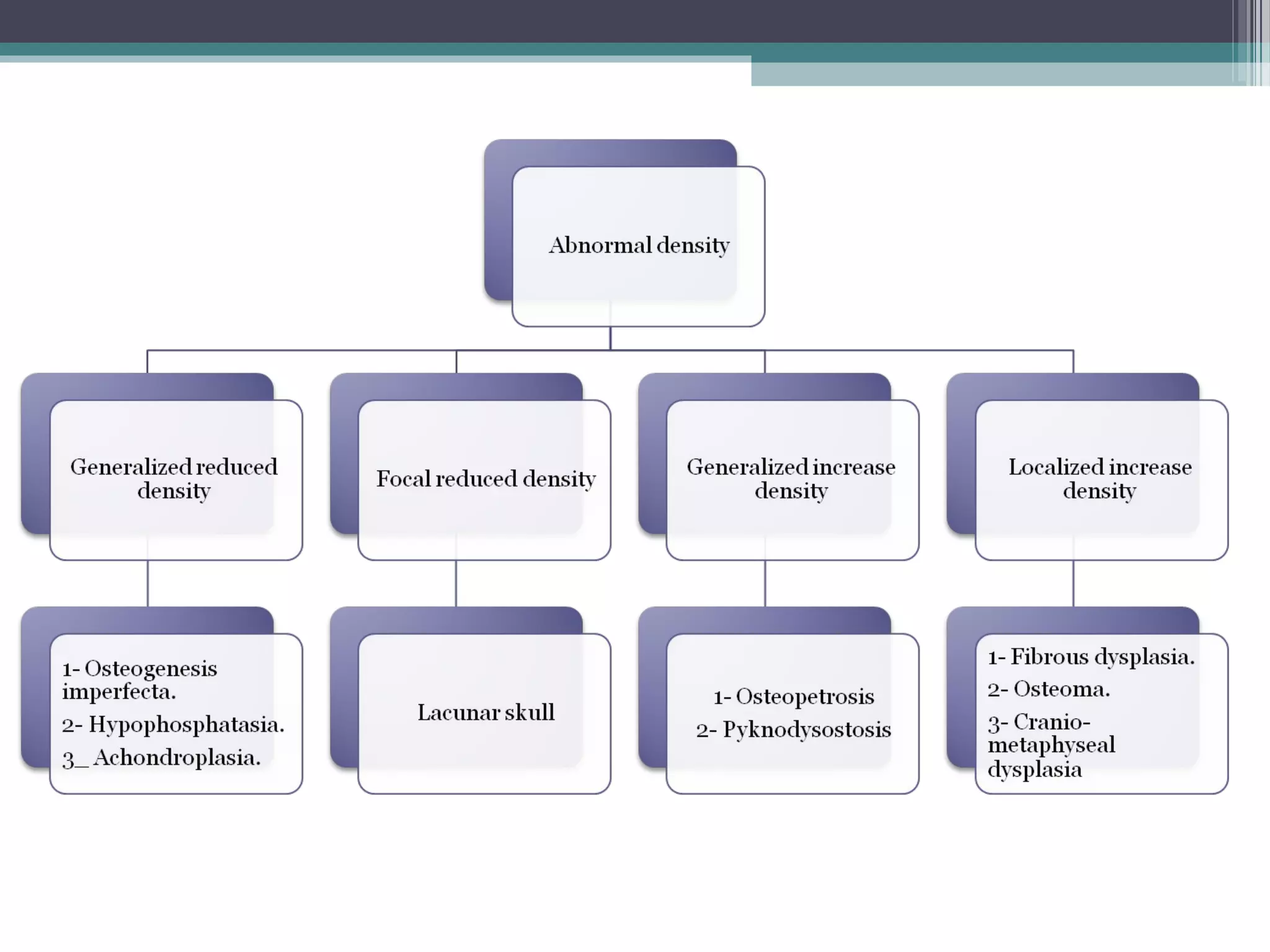
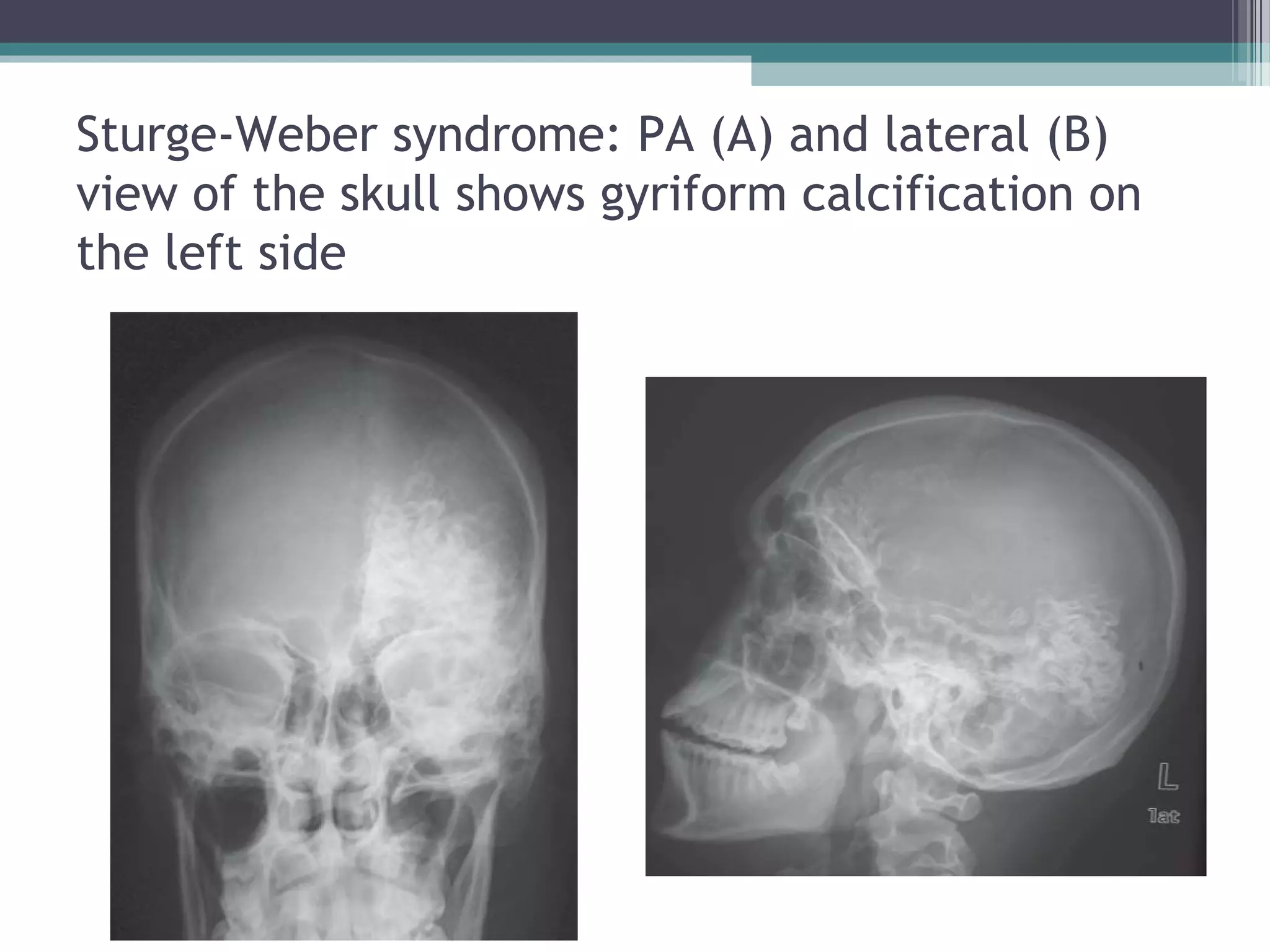

This document provides an overview of skull anatomy and evaluation of plain x-rays of the skull. It describes the bones that make up the skull and their sutures and fontanelles. It outlines the indications for skull x-rays including evaluation of skeletal dysplasias, infections, tumors and metabolic bone diseases. Common x-ray views of the skull are described including lateral, frontal, Towne's and basal views. Abnormal findings on skull x-rays can include changes in density, contour, intracranial volume, calcifications and lucent defects. Specific conditions like craniosynostosis, anemia and fractures are discussed.


































![Introduction to skull[1]](https://cdn.slidesharecdn.com/ss_thumbnails/introductiontoskull1-170504174910-thumbnail.jpg?width=640&height=640&fit=bounds)



![Radiography of skull [Autosaved].pptxriuyowioehgg](https://cdn.slidesharecdn.com/ss_thumbnails/radiographyofskullautosaved-251211014507-1d75cfe3-thumbnail.jpg?width=640&height=640&fit=bounds)