Downloaded 2,293 times
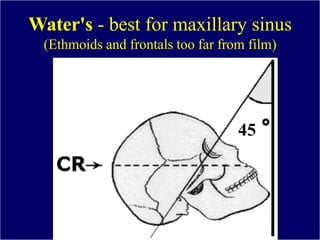



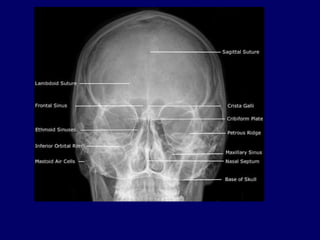



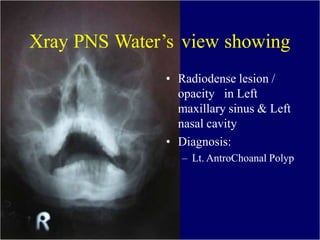




























































This document provides information on various radiographic views and examinations of the head and neck region. It discusses Water's view for imaging the maxillary sinuses, basic positioning for paranasal sinus views, Caldwell's view for the ethmoid and frontal sinuses, and examples of common sinus findings on radiography like mucosal thickening and retention cysts. It also summarizes techniques for imaging the nasopharynx, neck, cervical spine, trachea, and larynx. Common foreign body locations and aspiration findings are outlined. Sialography for salivary gland evaluation and bronchography are briefly described. Finally, it reviews skull radiographic views like PA, Caldwell, Chamberlain-Townes, and lateral projections as

















































































