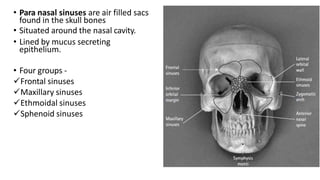
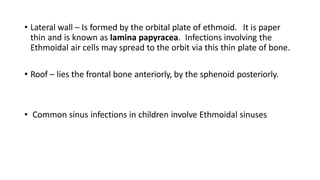
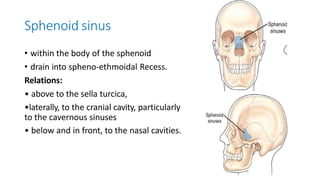
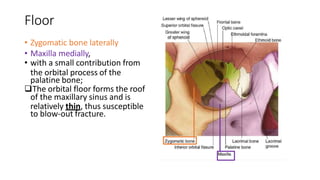
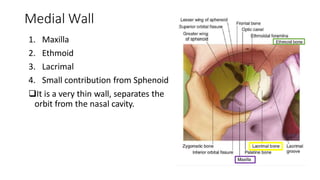
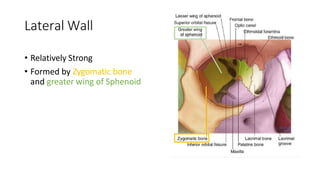
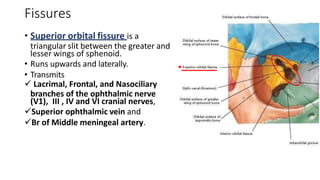
This document describes the anatomy and x-ray imaging of the paranasal sinuses and orbit. It details the four groups of paranasal sinuses - frontal, maxillary, ethmoidal, and sphenoidal. It explains their functions and anatomical features. Maxillary sinus anatomy and relations are described in detail. Common sinus infection sites in children involve the ethmoidal sinuses. X-ray views for examining the paranasal sinuses include Waters, Caldwell, and lateral views. Orbital anatomy includes bones forming the roof, floor, medial and lateral walls, and fissures like the superior and inferior orbital fissures.

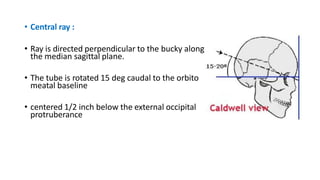
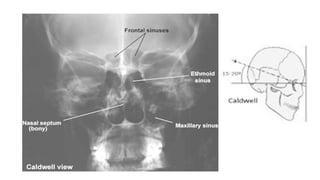
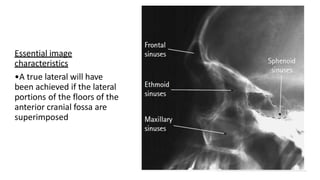
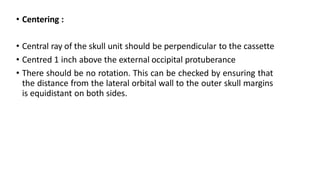
![Caldwell view [occipito frontal with 15 deg caudad]
• This projection is used to demonstrate the frontal
and ethmoid sinuses.
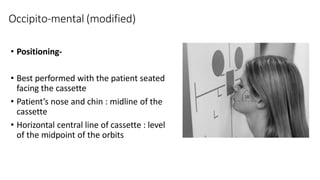
• Positioning of patient :
• Patient is seated facing the erect bucky
• Neck is flexed to bring nose and forehead in contact
with the bucky.
• orbito meatal line perpendicular to the bucky,](https://image.slidesharecdn.com/x-raypns-221115174740-8760515a/85/X-RAY-PNS-pptx-19-320.jpg)










































![Radiography of skull [Autosaved].pptxriuyowioehgg](https://cdn.slidesharecdn.com/ss_thumbnails/radiographyofskullautosaved-251211014507-1d75cfe3-thumbnail.jpg?width=640&height=640&fit=bounds)













































