Downloaded 29 times

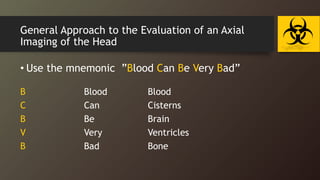
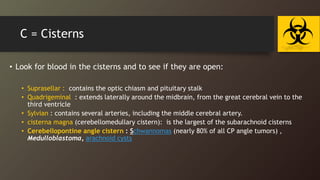
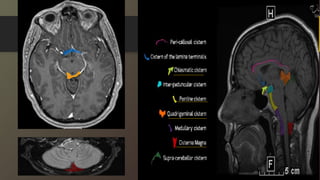
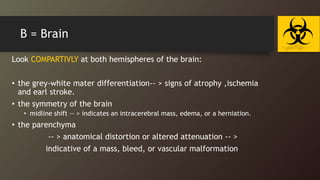
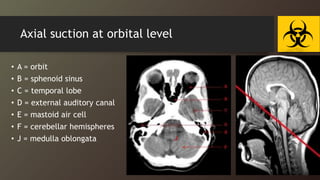
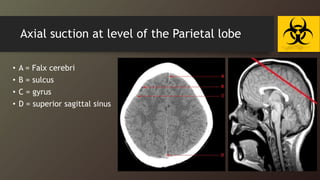
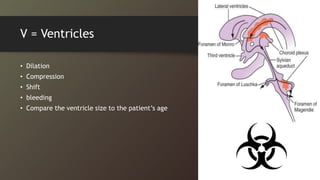
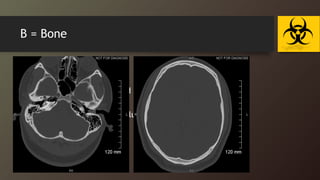



This document provides an overview of head and brain CT imaging. It discusses the basics of CT imaging, indications for head CT, and an approach to interpreting brain CT scans. The approach involves examining images for blood, cisterns, brain tissue, ventricles, bone, and other areas. Key anatomy is identified on various axial image slices. Several case examples are also presented and discussed.