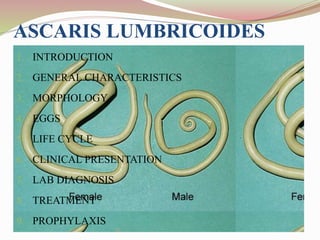
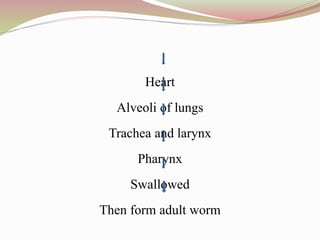
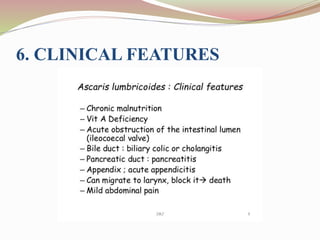
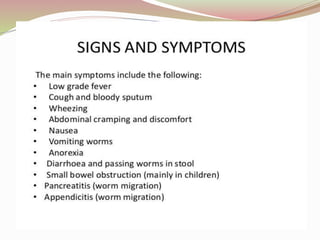
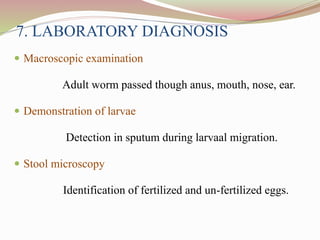
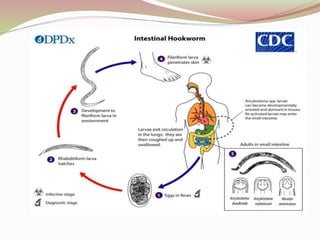
The document provides a detailed overview of intestinal nematodes, focusing on their characteristics, life cycles, and specific types like Ascaris lumbricoides and Ancylostoma duodenale. It discusses their morphology, modes of transmission, clinical features, laboratory diagnosis, treatment, and preventive measures. Nematodes are described as thread-like structures with separate sexes, and the document highlights the prevalence of these infections, particularly in underdeveloped regions.