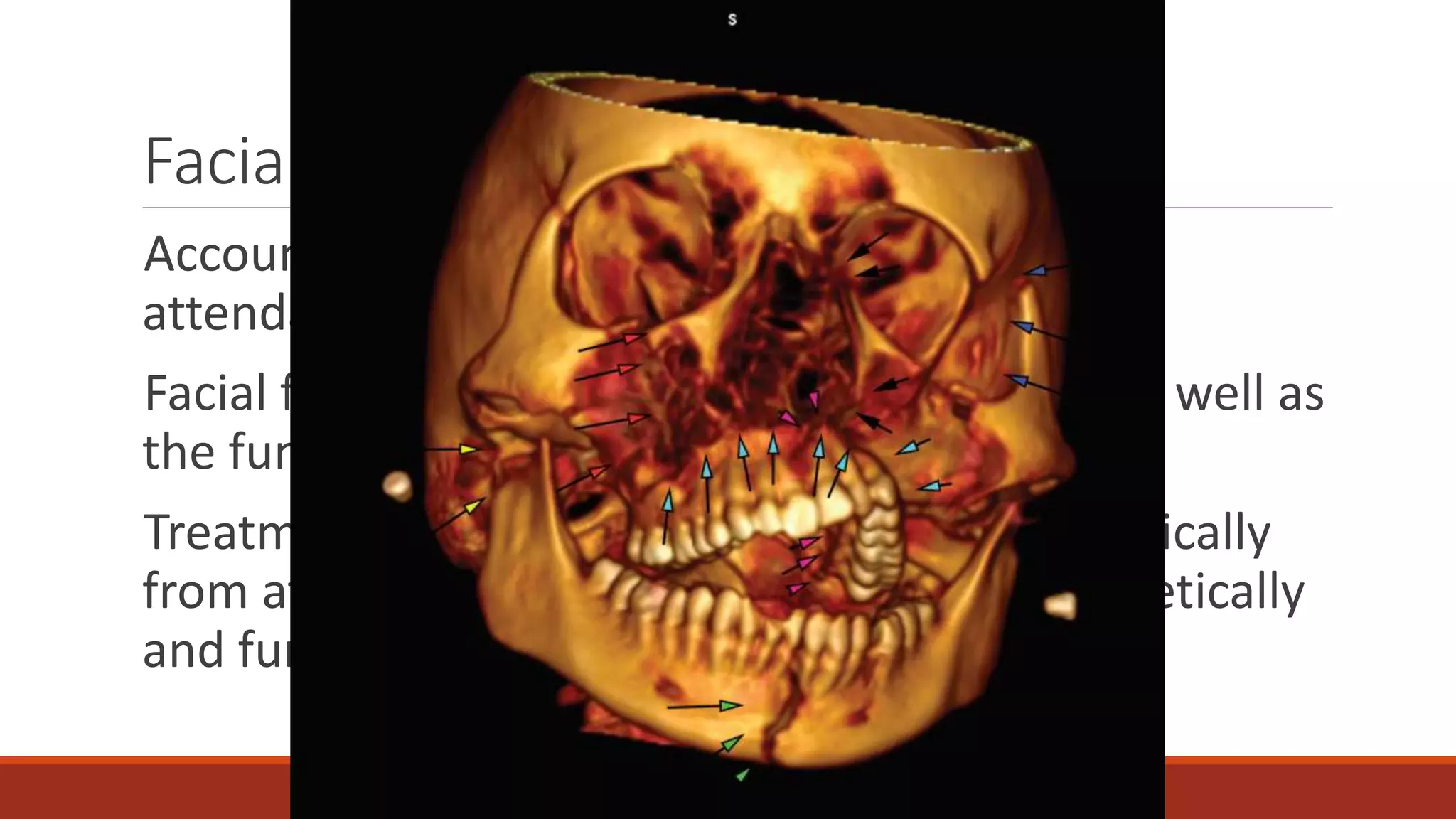
Facial fractures account for 10% of accidents and emergency department attendance. Treatment has changed from focusing only on dental occlusion to achieving aesthetically and functionally normal facial structure. Initial management involves stabilizing airway, breathing, circulation, disability and exposure. Further evaluation includes classifying fracture pattern and extent of injury through physical exam and imaging. Common fractures include nasal, mandible, maxilla, zygomatic, and orbital floor. Management depends on fracture type but often involves closed or open reduction with fixation using plates, screws or wires. Complications can include infection, malunion or restricted movement.