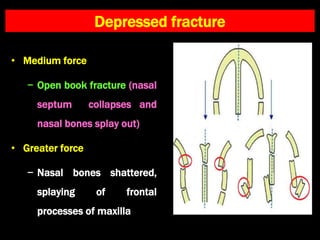
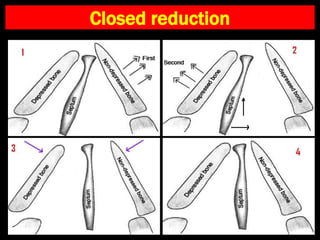
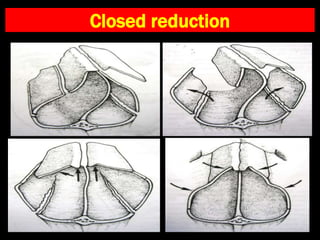
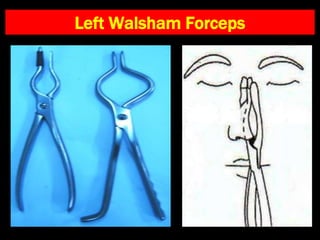
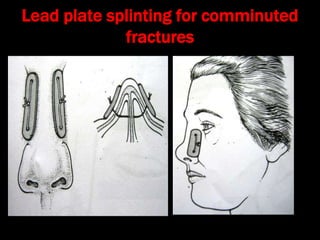
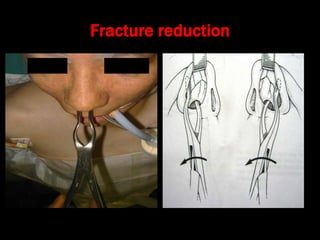
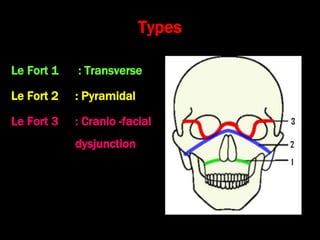
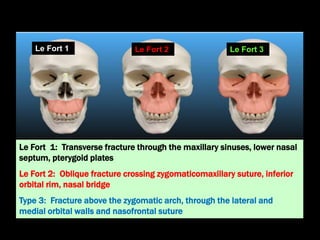
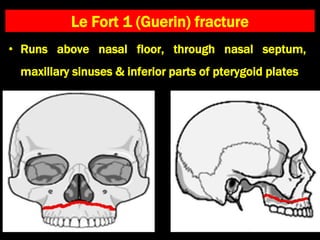
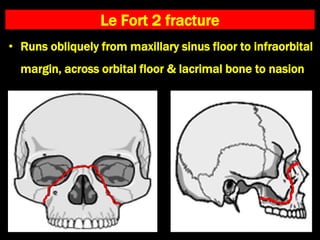
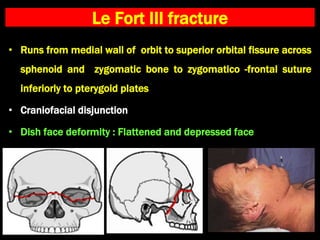
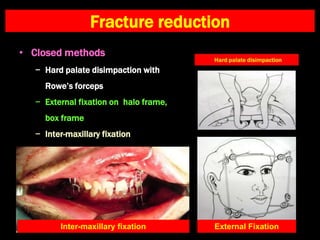
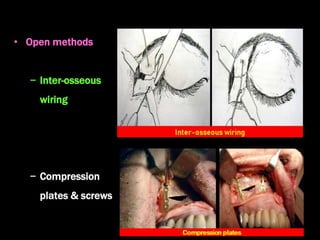
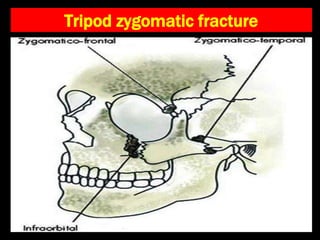
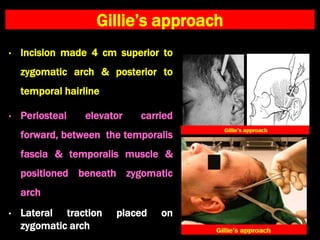
The document discusses facial bone fractures, highlighting nasal bone fractures as the most common type and outlining their management based on various causes like accidents and assaults. It details examination techniques for assessing facial injuries, classification of nasal fractures, and treatment protocols including closed and open reduction methods. Additionally, it covers related fractures, such as Le Fort fractures and mandible fractures, providing guidance on detection and their specific management strategies.