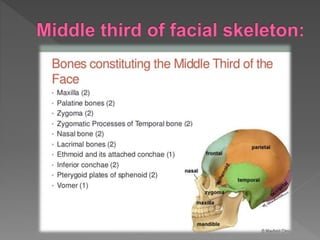
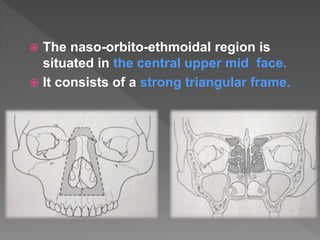
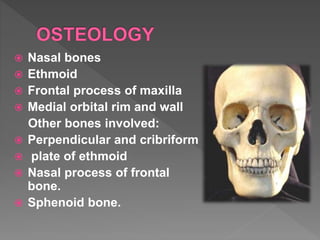
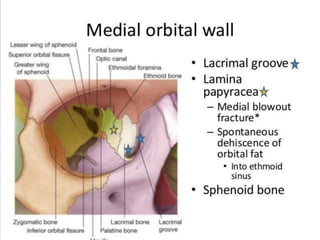
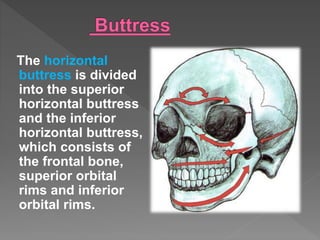
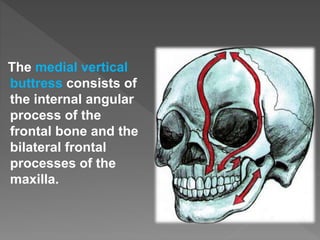
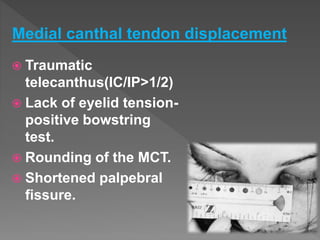
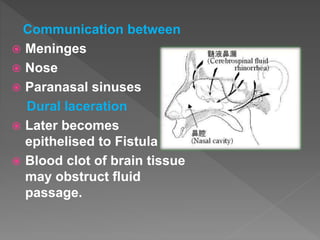
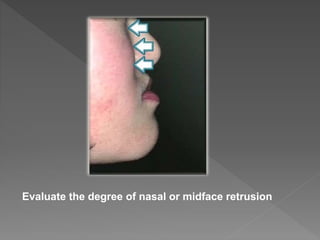
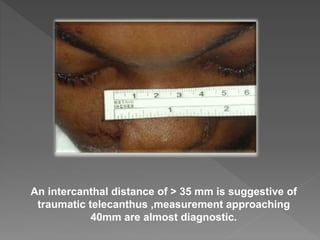
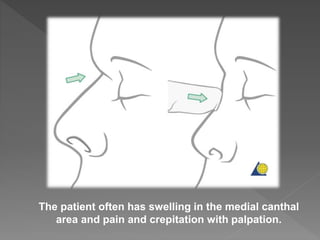
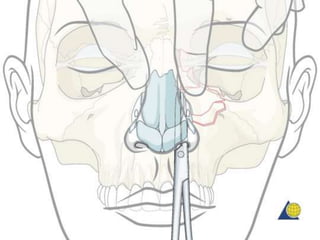
The naso-orbito-ethmoidal (NOE) region consists of a complex of delicate bones that form the central upper midface. Fractures in this region can be challenging to manage due to the anatomy. The NOE region contains four cavities and is reinforced by vertical and horizontal buttresses. It is supplied by arteries and innervated by branches of the trigeminal nerve. Clinical evaluation of NOE fractures involves examining for signs of injuries to the nose, eyes, medial canthal tendon, and possible intracranial involvement. Classification systems help determine fracture patterns and guide management.
























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
