Downloaded 381 times
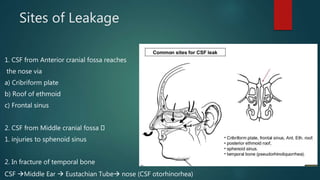
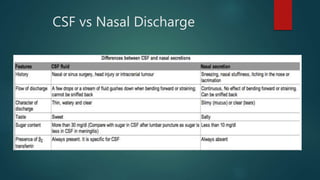

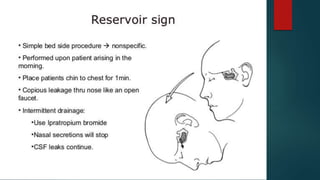


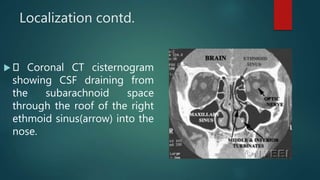

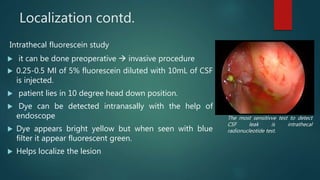
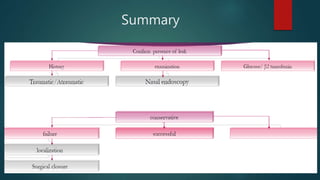


The document discusses cerebrospinal fluid (CSF) rhinorrhea, including its physiology, causes, and clinical presentation. It outlines the diagnosis through various tests and imaging techniques, as well as management strategies, both conservative and surgical. It emphasizes the importance of identifying the site of CSF leakage for effective treatment.



































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)