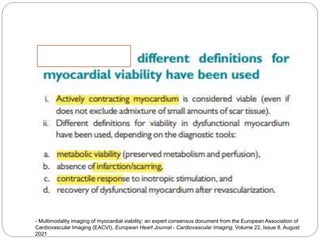
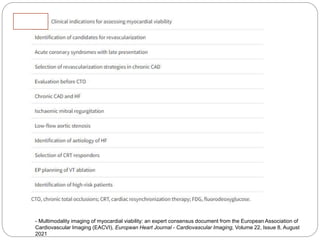
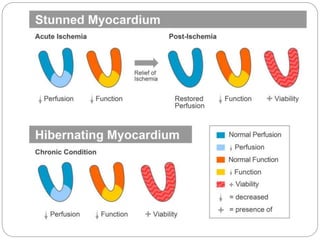
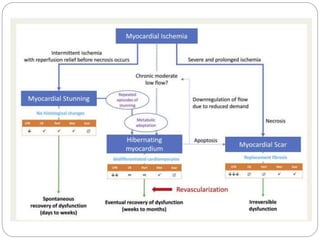
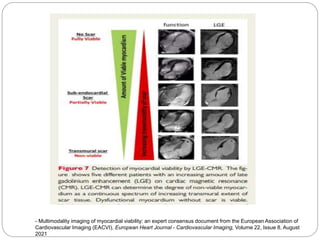
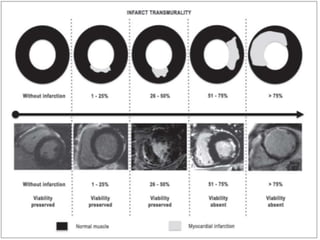
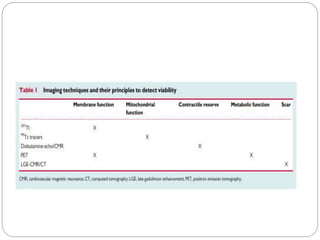
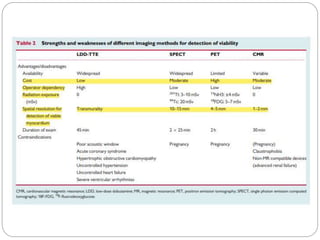
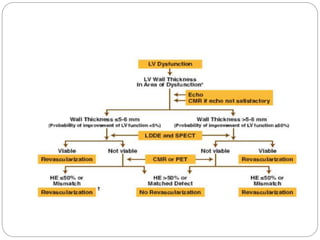
The document discusses the assessment of myocardial viability, emphasizing the importance of identifying viable myocardium in patients with left ventricular dysfunction due to coronary artery disease. It outlines various pathophysiological states of myocardium such as stunned, hibernating, and non-viable myocardium, and reviews multiple imaging modalities, including echocardiography, SPECT, PET, and cardiac MRI, for viability testing. The consensus highlights that timely reperfusion can restore contractility in viable myocardium, and detailed assessment of perfusion and metabolism is crucial for effective treatment decisions post-myocardial infarction.