Downloaded 399 times


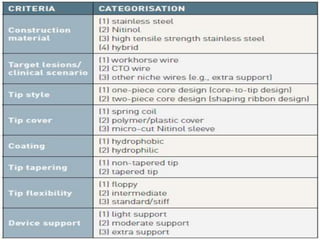
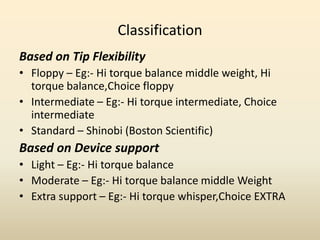




This document discusses coronary guidewires used in percutaneous coronary intervention (PCI). It begins by outlining the history of angioplasty and guidewire development. It then covers the purpose, components, classifications, and appropriate uses of guidewires. The main components include the core, tip, coils, covers, and coatings. Guidewires are classified based on flexibility, device support, and clinical usage. Complications like vessel perforation, pseudolesions, and entrapment are also discussed. Proper guidewire manipulation and strategies for difficult lesions are outlined to maximize safety and efficacy.












































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
