Screening
It is amethod for detecting disease
or body dysfunction before an
individual would normally seek
medical care.
4.
Screening for referralin Physical Therapy
It is the Therapist’s responsibility is to have an
appropriate patient for physical therapy
In order to be Cost effective…we must determine
NMS dysfunction…Treat specifically
PT must be able to identify sign and symptoms of
systemic disease that can mimic neuromuscular or
musculoskeletal dysfunction…shoulder and back
pain
Cancer is major part of medical screening
5.
Reason for MedicalDisease Screening
Direct access
Quicker & sicker
Signed prescription
Medical specialization
Progression of time & disease
Patient /client disclosure
Presence of one or more yellow or red flags
6.
DIRECT ACCESS
Directaccess is the right of the public to obtain
examination , evaluation, and
intervention from a licensed physical therapist
with out previous examination by, or referral
from, a physician , or other practitioner.
7.
Signed Prescription
clientsmay obtain a signed prescription for
physical therapy from their primary care
physician or other health care provider, based on
similar past complaints of musculoskeletal
symptoms, without actually seeing the physician
or being examined by the physician.
8.
F o ll o w - U p Questions
Always ask a client who provides a signed
prescription:
• Did you actually see the physician
(chiropractor,dentist, nurse practitioner,
physician assistant)?
Did the doctor (dentist) examine you?
9.
Case 1-1
Apatient visited physiotherapy clinic with signed prescription of
physician without detailed examination. Actually the patient had
telephonic conversation with physician and described the same
previous pain history and recovery with physiotherapy.
The patient presented with hip and bilateral leg pain , during
examination it is observed that there is swelling in both legs,
chest pain and low blood pressure. There is also history of heart
disease.
What would be the next step of therapist?
What treatment options?
What is the most appropriate way to handle this situation?
10.
Suggestions:
Good ideais to call
Best idea is to write a brief but complete
report.
Highlight significant findings: B/L edema, low
BP that day…
Open ended comment like “please advice” or
what do u think
Some physician ask for your opinion.
11.
Medical Specialization
Withincreasing specialization of medicine, client
evaluated by Medical specialists who does not
immediately recognize underlying systemic
disease.
or the specialist may assume that the referring
primary care physician has ruled out other
causes
Progression of Timeand Disease
In some cases, early signs and symptoms of
systemic disease may be difficult or impossible to
recognize until the disease has progressed
enough to create distressing or noticeable
symptoms
Case 1-3
17.
Quicker and Sicker
"Quicker" refers to how health care delivery has
changed in the last 10 years to combat the rising
costs of health care.
The therapist must be alert to red flags of
systemic disease at all times but especially in
those clients who have been given early release
from the hospital or transition unit.
18.
Cont…
"Sicker" refersto the fact that patient/clients in acute
care, rehabilitation, or outpatient/client setting with
any orthopedic or neurologic problems may have a
past medical history of cancer or a current personal
history of diabetes, liver disease, thyroid condition,
peptic ulcer, and/or other conditions or diseases.
So, the need to view the whole patient and not just
the body part in question.
19.
Patient/Client Disclosure
Finally,sometimes p a t i e n t / c l i e n t s tell the
therapist things about their current health and
social h i s t o r y
u n k n o w n or u n r e p o r t e d to the physician.
20.
Yellow or RedFlags
A yellow flag is a cautionary or warning
symptom that signals " slow down" and think
about the need for screening.
A red-flag symptom requires immediate
attention , either to pursue further screening
questions and/or tests , or to make an
appropriate referral .
21.
RED flags
Factorsthat require immediate medical attention
- Blood in sputum
- LOC or altered mental status
- Neurological deficit not explained by
monoradiculopathy
- Numbness or paresthesia in the perianal region
(aka saddle anesthesia)
- Pathological changes in bowel and bladder
- Patterns of symptoms not compatible with
mechanical pain (on physical exam)
- Progressive neurological deficit
- Pulsatile abdominal mass (AAA)
22.
Yellow Flags
Depression
oScreened for within general health
questionnaire and followed-up with physical
therapist if considered positive
“
During the past month, have you often been
bothered by feeling down,
depressed, or hopeless?”
“
During the past month, have you often been
bothered by little interest or
pleasure in doing things?”
- Anxiety
- Malingering/Non-Organic Pain
23.
Past Medical History
• Personal or family history of cancer
• Recent (last 6 weeks) infection
Recent history of trauma such as motor
vehicle accident or fall (fracture; any age) or
minor trauma in older adult with
osteopenia/osteoporosis
• History of immunosuppression (e.g.,
steroids, organ transplant, HIV)
• History of injection drug use (infection
24.
Risk Factors
Substanceabuse
Tobacco use
Sedentary lifestyle
Age
Obesity
Gender
Domestic violence
25.
Clinical Presentation
Noknown cause/insidious onset
Cyclical presentation:Better/worse/better
Weight loss/gain within 10-21days
Unrelieved by rest/positional change
Unrelieved by PT intervention
Persist longer than expected
Growing mass
Unable to alter symptoms during examination
26.
Cont…
Postmenopausal vaginalbleeding
Bilateral symptoms:
Edema
Numbness/tingling
Clubbing
Skin rash
Change in muscle tone or ROM for individuals
with neurological symptoms (CP, SCI, TBI, MS)
27.
Pain pattern
Backor shoulder pain
Pain with full and painless ROM
Night pain
Constant and intense
Poorly localized
Vascular/ neurological/ musculoskeletal/
emotional
28.
Associated Signs and
Symptoms
Recent report of confusion (or increased
confusion
Presence of constitutional symptoms
Proximal muscle weakness, especially if
accompanied by change in DTRs
Joint pain with skin rashes, nodules
Important Question toend
Are there any symptom anywhere else in your
body that may not seem related to your current
problem??
31.
Physical Therapist Rolein
Disease Prevention
Primary Prevention:
Stopping the processes) that lead to the development of diseases),
illness(es), and other pathologic health conditions through
education, risk-factor reduction, and general health promotion
Secondary Prevention:
Early detection of disease(es), illnesses), and other pathologic
health conditions through regular screening; this does not
prevent the condition but may decrease duration and/or severity
of disease and thereby improve the outcome, including improved
quality of life
Tertiary Prevention:
Providing ways to limit the degree of disability while improving
function in patients/clients with chronic and/or irreversible
diseases
32.
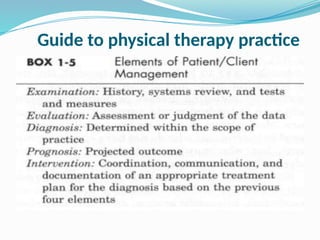
DIAGNOSIS BY THE
PHYSICALTHERAPIST
It is the policy of the (APTA) that PT shall
establish a diagnosis for each patient.
PTs use diagnostic labels that i d e n tify the
impact of a condition on function at the level of
the system (especially the movement system)
and the level of the whole person.
The PT is qualified to make a diagnosis
regarding primary NMS conditions though we
must do so in accordance with the state practice
act.
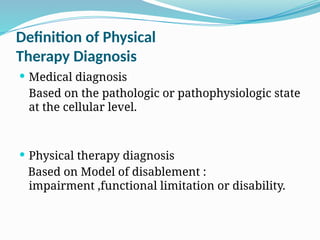
Definition of Physical
TherapyDiagnosis
Medical diagnosis
Based on the pathologic or pathophysiologic state
at the cellular level.
Physical therapy diagnosis
Based on Model of disablement :
impairment ,functional limitation or disability.
37.
Diagnosis ???
Alabel encompassing a cluster of sign & symptoms
commonly associated with a disorder or syndrome
or category of impairment ,functional limitation or
disability.
38.
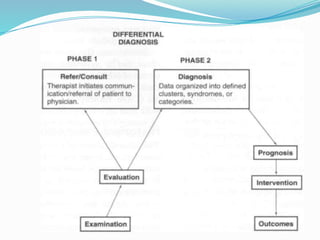
Differential diagnosis
Aprocess of identifying all of the possible
diagnoses that could be connected to the signs,
symptoms, and lab findings, and then ruling out
diagnoses until a final determination can be
made.
List of diagnosis
39.
Purpose of theDiagnosis
Treat as specifically as possible by determining
the most appropriate intervention strategy for
each patient / client
Recognize the need for a medical referral
40.
Case referral
Referral. A32-year-old female university student was referred for physical
therapy through the student health service 2 weeks ago. The physician's
referral reads: "Possible right oblique abdominis tear/possible right
iliopsoas tear.
" A faculty member screened this woman initially, and the diagnosis was
confirmed as being a right oblique abdominal strain.
History. Two months ago, while the client was running her third mile, she felt
"severe pain" in the right side of her stomach. She felt immediate nausea
and had abdominal distension.
She cannot relieve the pain by changing the position of her leg. Currently, she
still cannot run without pain.
41.
Presenting Symptoms. Painincreases during sit-ups, walking
fast, reaching, turning, and bending. Pain is eased by heat
and is reduced by activity. Pain in the morning versus evening
depends on body position. Once the pain starts, it is
intermittent and aches.
The client describes the pain as being severe, depending on her
body position. She is currently taking aspirin when necessary.
42.
SAMPLE LETTER
John Smith,M.D.
University of Montana Heolth Service
Eddy Street
Missoula, MT59812
Re: Jone Doe
Dear Dr. Smith,
Your client, Jane Doe, was evaluated in our clinic on 5 / 2 / 0 6 with the
following pertinent findings:
Subjective. She has severe pain in the right lower abdominal quadrant
associated with nausea and abdominal distension Although the onset of
symptoms started while the client was running, she denies any precipitating
trauma. She describes the course of symptoms as having begun 2 months ago
with temporary resolution and now with exacerbation of earlier symptoms.
Additionally, she reports chronic fatigue and frequent night sweats.
43.
Objective. Presenting painis reproduced by resisted hip or
trunk flexion with accompanying tenderness/tightness on
palpation of the right iliopsoas muscle (compared with the
left iliopsoas muscle). There are no implicating neurologic
signs or symptoms,
Assessment. A musculoskeletal screening examination is
consistent with your diagnosis of a possible iliopsoas or
abdominal oblique tear.
Jane appears to have a combination of musculoskeletal and
systemic symptoms, such as those outlined earlier. Of
particular concern are the symptoms of fatigue, night sweats,
abdominal distension, nausea, repeated episodes of
exacerbation and remission, and severe quality of pain and
location (right lower abdominal quadrant].
These symptoms appear to be of a systemic nature rather than
caused by a musculoskeletal lesion.
44.
Recommendations. I suggestthat the client return to you for further medical
follow-up to rule out any systemic involvement before the initiation of
physical therapy services. I am concerned that my proposed intervention of
ultrasound, soft tissue mobilization, and stretching may aggravate an
underlying disease process.
I will contact you directly by telephone by the end of the week to discuss
these findings and to answer any questions that you may have.
Thank you for this interesting referral.
Sincerely,
Catherine C. Goodman, M.B.A., P.T.
R e s u l t . This client returned to the physician, who then ordered laboratory
tests. After an acute recurrence of the symptoms described earlier, she had
exploratory surgery. A diagnosis of a ruptured appendix and peritonitis was
determined at surgery. In retrospect, the proposed ultrasound and soft tissue
mobilization would have been contraindicated in this situation.

![Objective. Presenting pain is reproduced by resisted hip or
trunk flexion with accompanying tenderness/tightness on
palpation of the right iliopsoas muscle (compared with the
left iliopsoas muscle). There are no implicating neurologic
signs or symptoms,
Assessment. A musculoskeletal screening examination is
consistent with your diagnosis of a possible iliopsoas or
abdominal oblique tear.
Jane appears to have a combination of musculoskeletal and
systemic symptoms, such as those outlined earlier. Of
particular concern are the symptoms of fatigue, night sweats,
abdominal distension, nausea, repeated episodes of
exacerbation and remission, and severe quality of pain and
location (right lower abdominal quadrant].
These symptoms appear to be of a systemic nature rather than
caused by a musculoskeletal lesion.](https://image.slidesharecdn.com/introtoscreening-250523002351-b917d847/85/introduction-to-screening-for-defferential-daignosis-pptx-43-320.jpg)





































![Lecture 25 Intermuscular sapces and axilla [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/lecture25intermuscularsapcesandaxillaautosaved-251110002658-47b36c78-thumbnail.jpg?width=640&height=640&fit=bounds)




























