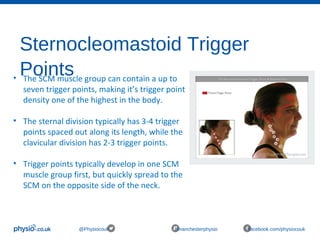
The document is a comprehensive outline for a workshop on trigger point therapy and soft tissue release aimed at sports and massage therapists, detailing its history, types, symptoms, and treatment techniques. It includes an itinerary, theory, practical sessions, indications, outcome measures, and precautions related to trigger point therapy. Additionally, it provides information on the formation of trigger points, their effects, and common contraindications during treatment.