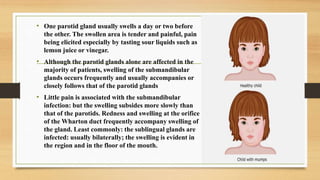
Mumps is a viral infection primarily affecting children, characterized by painful swelling of the salivary glands, particularly the parotids, and can lead to complications such as orchitis and meningitis, particularly in adults. The mumps virus spreads through respiratory secretions and is largely preventable through vaccination, with the MMR vaccine showing high efficacy. Key symptoms include parotid swelling, fever, and sometimes complications like pancreatitis; treatment is mostly supportive as no specific antiviral therapies exist.















































![Mumps[1]](https://cdn.slidesharecdn.com/ss_thumbnails/mumps1-200930140514-thumbnail.jpg?width=640&height=640&fit=bounds)