Downloaded 238 times








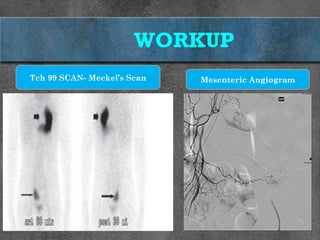









Meckel's diverticulum is a congenital anomaly resulting from the failure of the vitelline duct to obliterate, commonly presenting with symptoms like bleeding and obstruction. It is most frequently diagnosed in children and often requires surgical intervention in symptomatic cases, with a variety of surgical techniques available. Diagnosis is primarily confirmed through technetium-99m pertechnetate scintigraphy and management depends on the presence of complications or symptoms.























































































