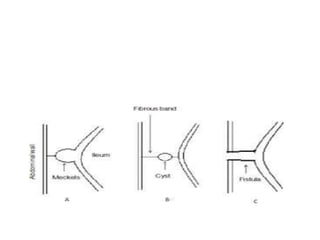
Meckel diverticulum is a congenital abnormality caused by persistence of the omphalomesenteric duct, which normally disappears by gestational week 9. It occurs in about 2% of the population and is most common in children under age 2. Complications include bleeding from ulceration caused by ectopic gastric tissue, intestinal obstruction, and diverticulitis. Symptoms include painless rectal bleeding in infants and intestinal obstruction presenting as vomiting and abdominal distension in newborns. Diagnosis involves scans concentrating isotopes in ectopic gastric mucosa or x-rays showing dilated bowel loops. Surgical removal of the diverticulum is treatment for complications like bleeding or obstruction.