Download to read offline















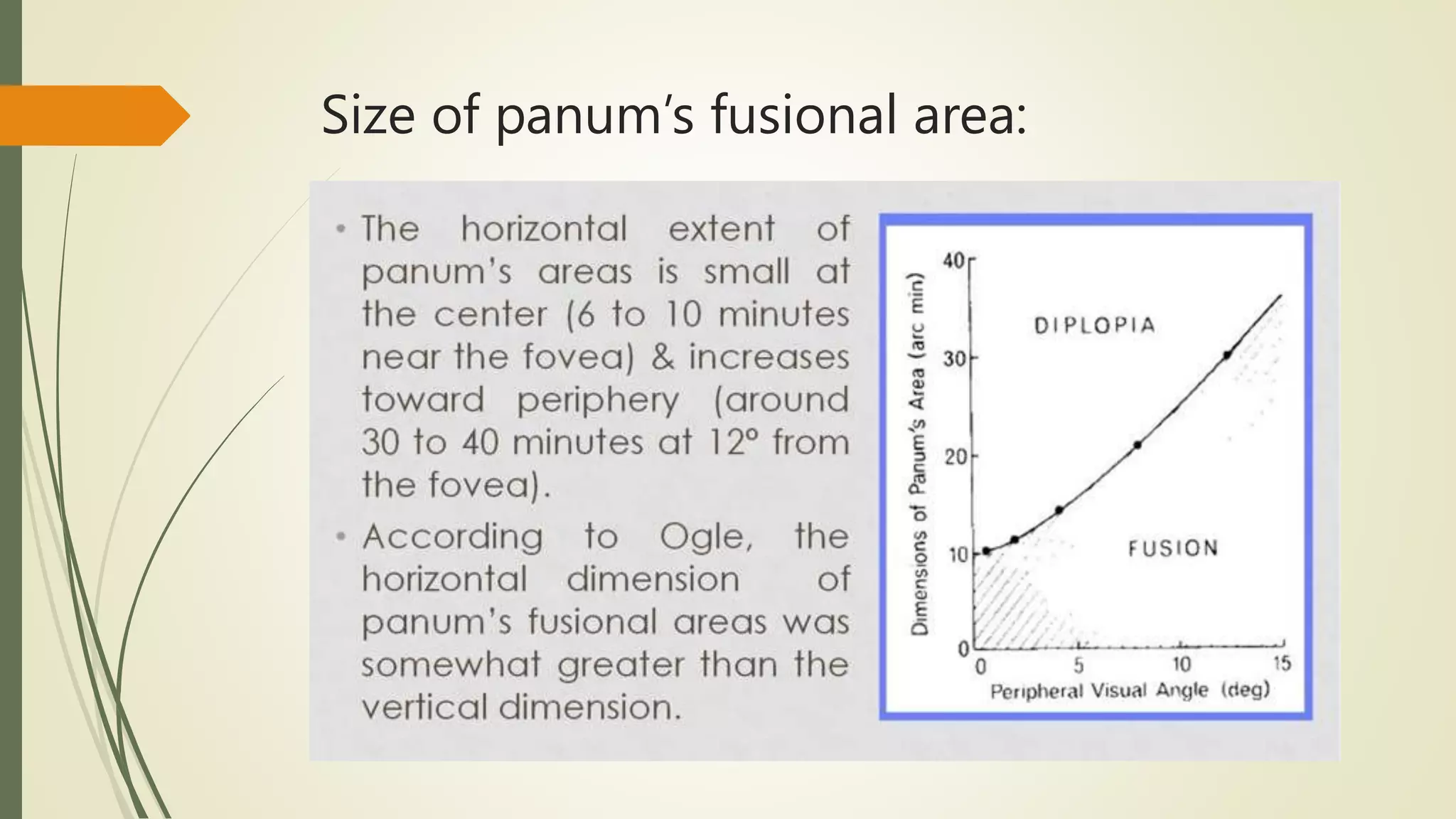


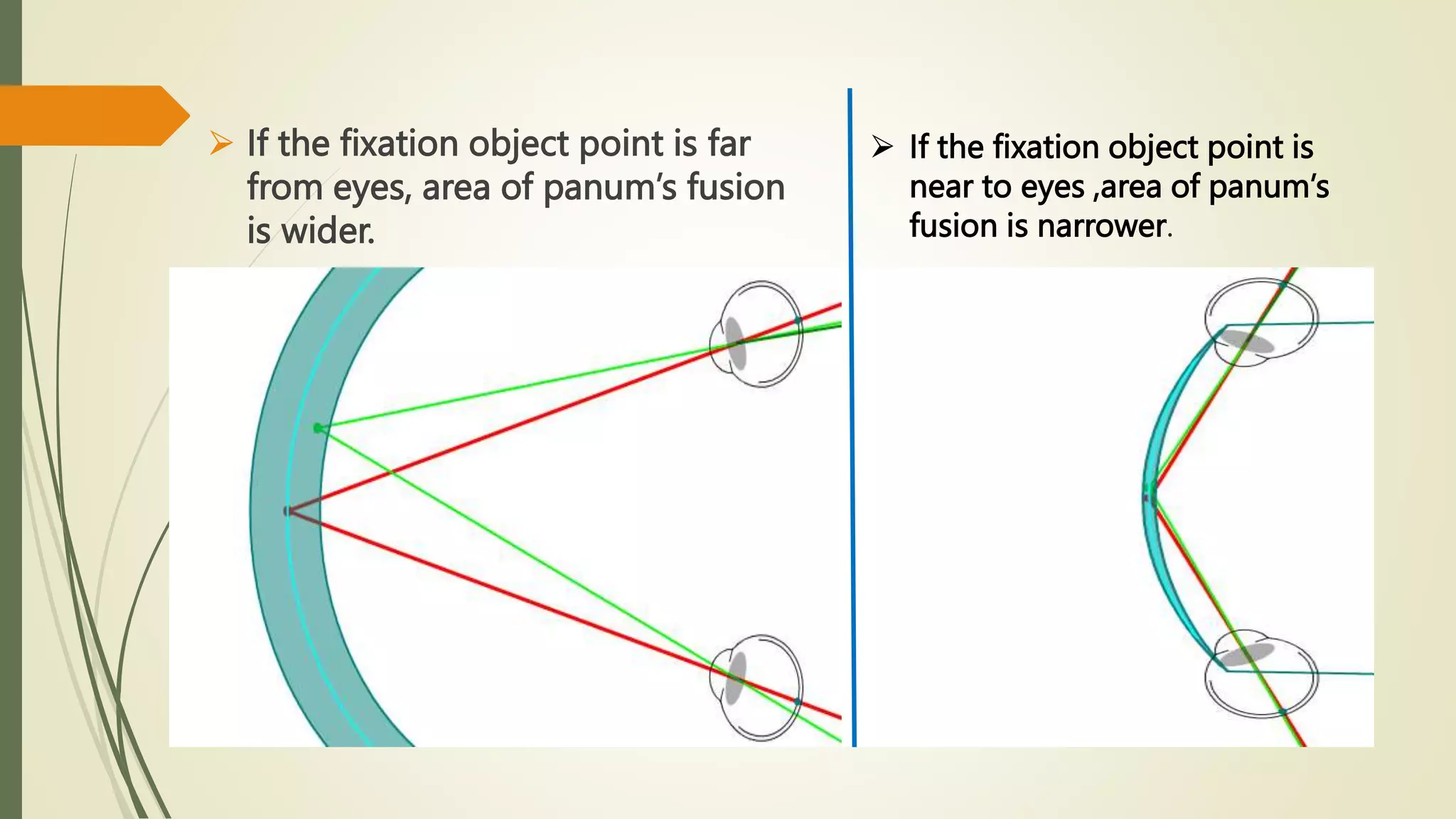
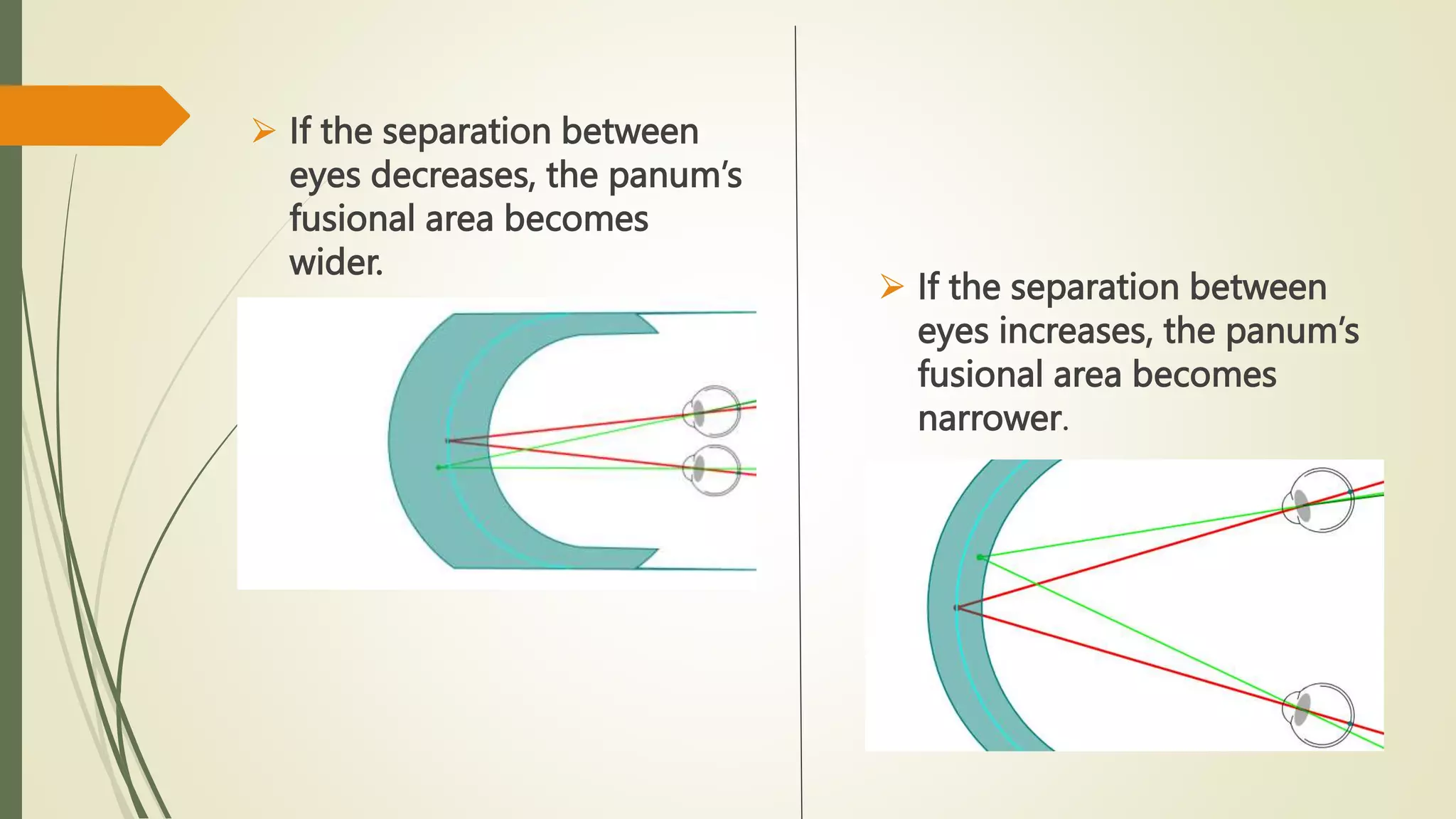
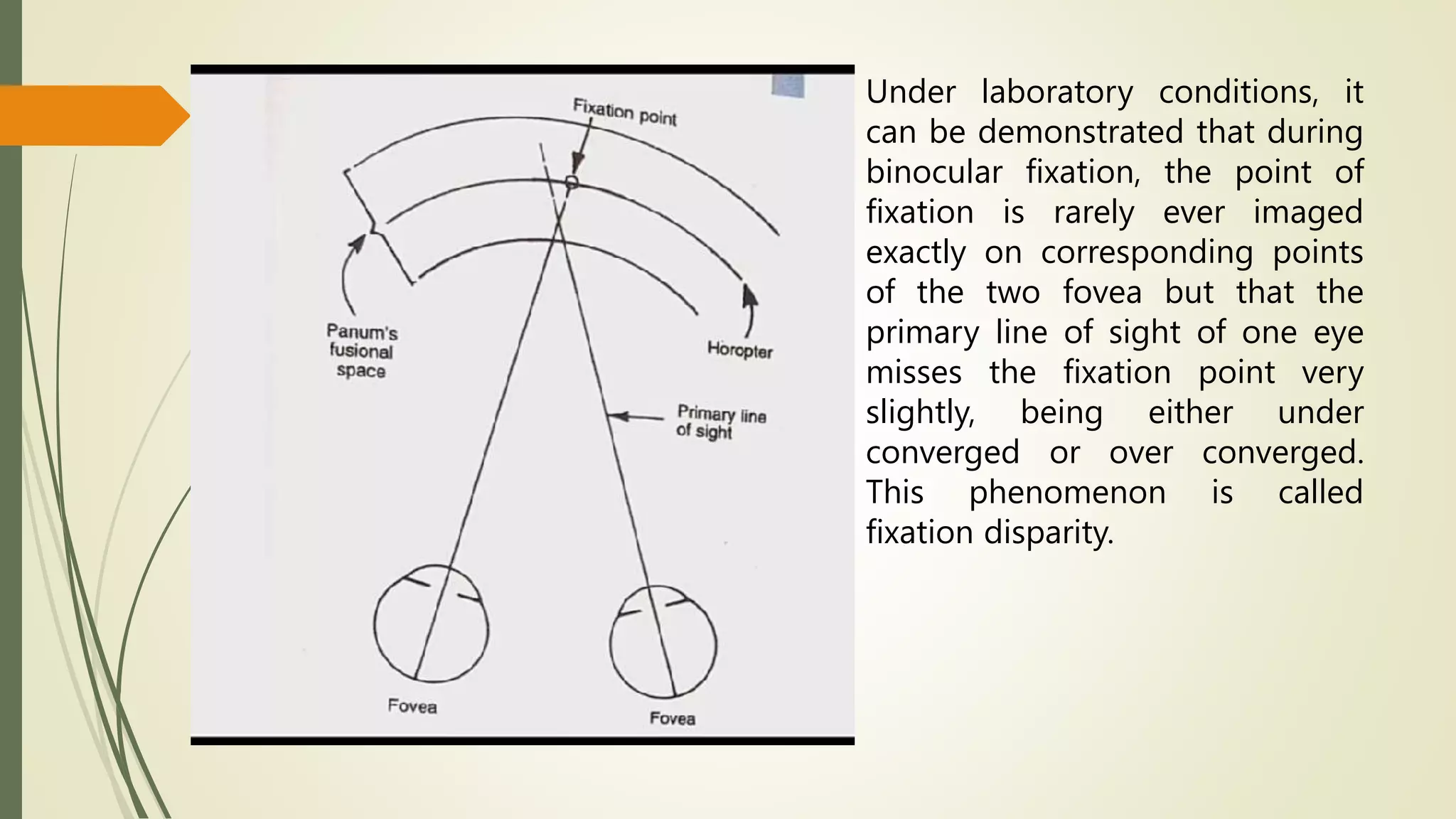


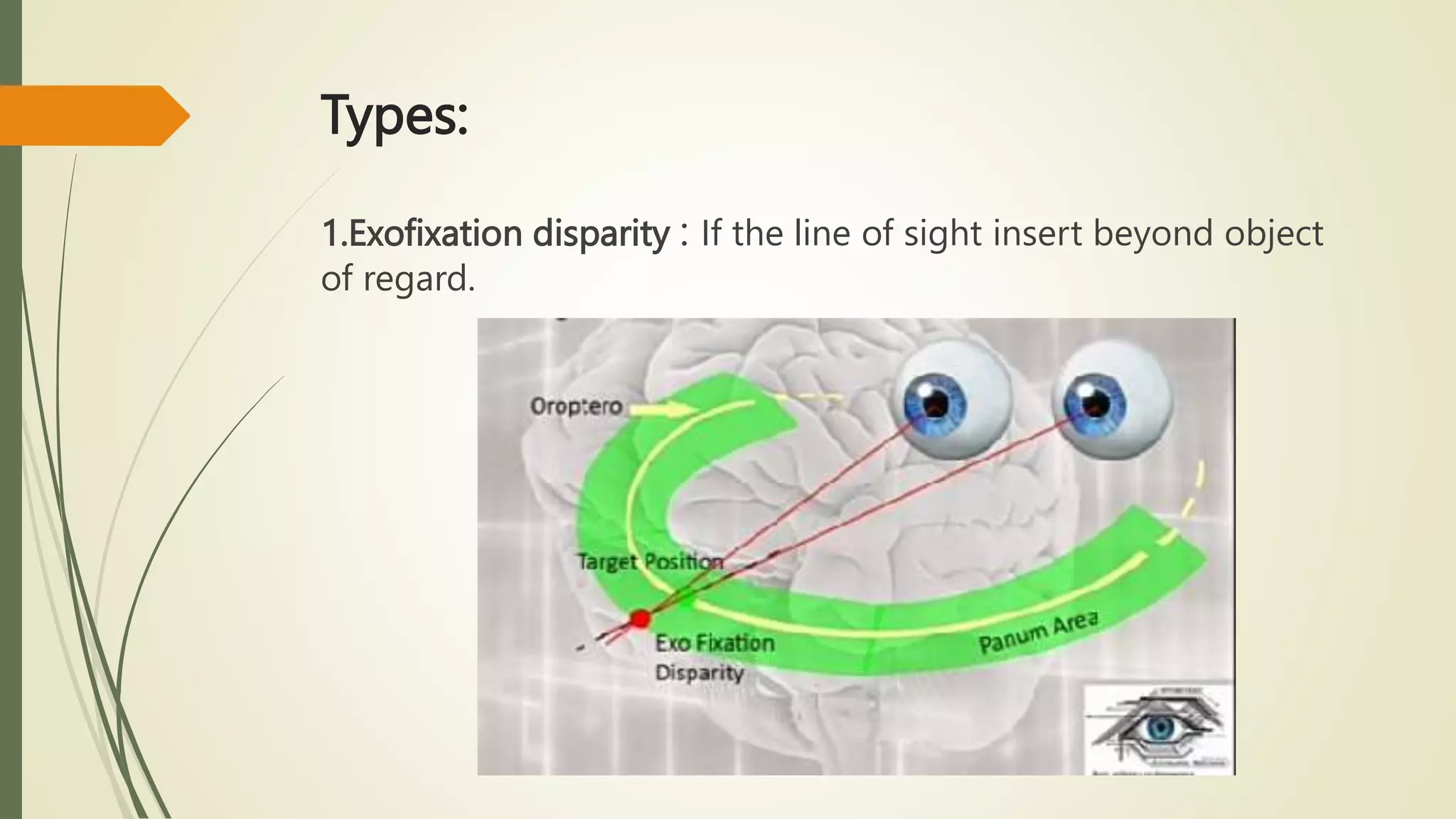













The document discusses various mechanisms and terminologies in binocular vision, including: - Corresponding retinal points, which allow for single binocular vision when stimulated. - The horopter, which is the locus of points that fall on corresponding retinal points. It can take different shapes depending on the fixation distance. - Panum's fusional area, which is the area around the horopter where binocular fusion can still occur. Its size depends on factors like fixation distance and interocular separation. - Fixation disparity, which is a small misalignment of the eyes during binocular fixation, usually horizontal or vertical, that does not cause diplopia due to being within Panum's area.



































































