Download to read offline

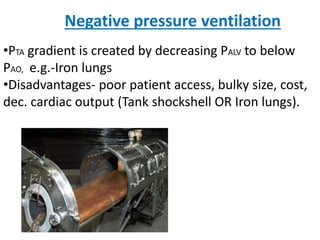
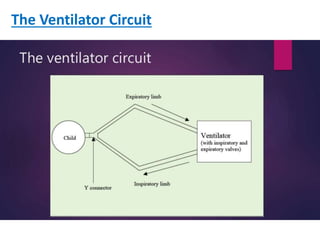
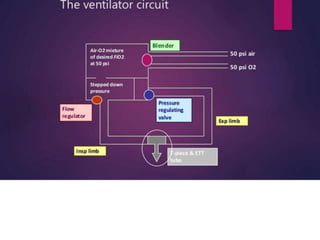
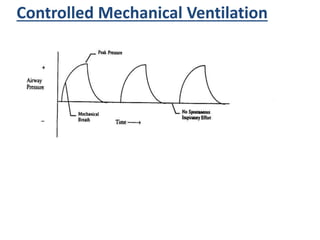
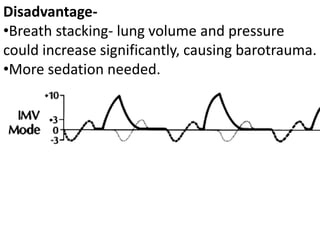
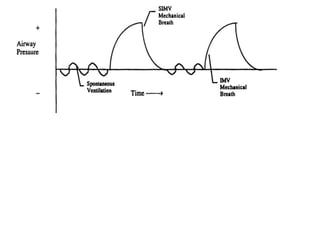


This document discusses different modes of mechanical ventilation. It begins by introducing mechanical ventilation and its purpose of providing respiratory support. It then describes the basic components of a ventilator and ventilator circuit. The document outlines several modes of mechanical ventilation including controlled mechanical ventilation, assist-control ventilation, intermittent mandatory ventilation, and synchronized intermittent mandatory ventilation. It provides details on the characteristics, advantages, and disadvantages of each mode.









































































