A L EK S A N D R A Š I L O V A , M F V I 4 . G R U P A
M E N T O R E : D R . G U N T A S U M E R A G A
Maligns ārējās auss iekaisums
2.
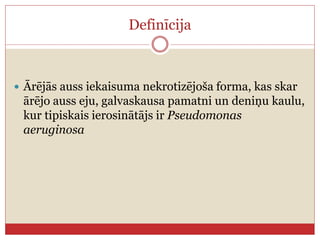
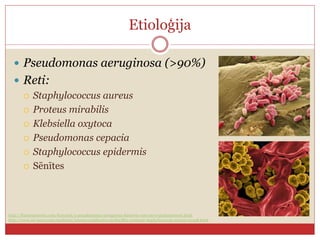
Definīcija
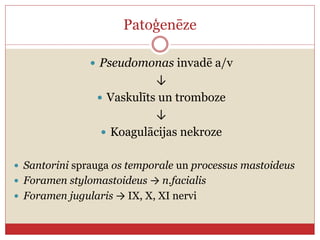
Ārējās aussiekaisuma nekrotizējoša forma, kas skar
ārējo auss eju, galvaskausa pamatni un deniņu kaulu,
kur tipiskais ierosinātājs ir Pseudomonas
aeruginosa
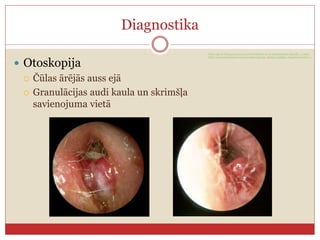
Diagnostika
Otoskopija
Čūlasārējās auss ejā
Granulācijas audi kaula un skrimšļa
savienojuma vietā
http://gpent.blogspot.com/2013/02/definition-oe-is-inflammatory-typically_11.html
http://eac.hawkelibrary.com/new/main.php?g2_itemId=353&g2_imageViewsIndex=1
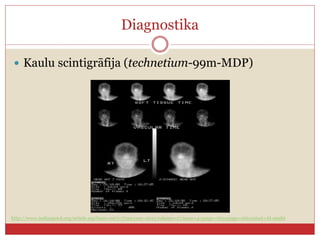
10.
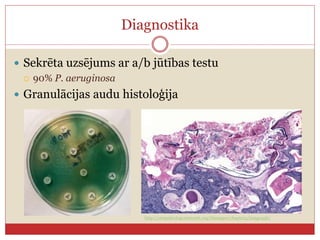
Diagnostika
Sekrēta uzsējumsar a/b jūtības testu
90% P. aeruginosa
Granulācijas audu histoloģija
http://otopathologynetwork.org/tbimages/chapter5/image436/
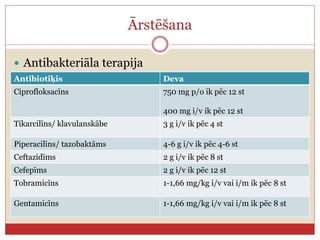
Ārstēšana
Antibakteriāla terapija
AntibiotiķisDeva
Ciprofloksacīns 750 mg p/o ik pēc 12 st
400 mg i/v ik pēc 12 st
Tikarcilīns/ klavulanskābe 3 g i/v ik pēc 4 st
Piperacilīns/ tazobaktāms 4-6 g i/v ik pēc 4-6 st
Ceftazidīms 2 g i/v ik pēc 8 st
Cefepīms 2 g i/v ik pēc 12 st
Tobramicīns 1-1,66 mg/kg i/v vai i/m ik pēc 8 st
Gentamicīns 1-1,66 mg/kg i/v vai i/m ik pēc 8 st
Pēc trīs mēnešiem
Drudzis
Nespēks
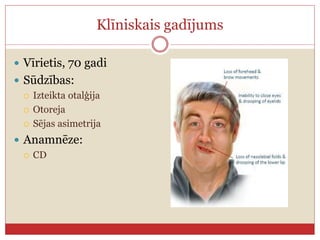
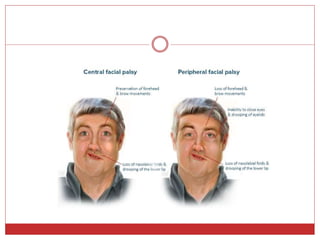
Sejas asimetrija
Rīšanas un runas traucējumi
Garšas traucējumi
Kādus nervus skara iekaisums?
VII, IX, un X kraniālie nervi
23.
Pēc trīs mēnešiem
Otalģija
Otoreja
Uzsējums - ciprofloksacīn-resistenta Pseudomonas
aeruginosa
Informācijas avoti
ProbstR. Grevers G. Iro H. Basic Otorhinolaryngology
A Step-By-Step Learning Guide. Georg Thieme Verlag,
2006
Handzel O, Halperin D., Necrotizing (Malignant)
External Otitis, Am Fam Physician. 2003 Jul 15;68(2):309-
312.
Sang Kuk Lee, Se A Lee, Sang Woo Seon, Jae Hyun Jung, Jong
Dae Lee, Jae Young Choi, Bo Gyung Kim, Analysis of
Prognostic Factors in Malignant External Otitis
Clinical and Experimental Otorhinolaryngology 2016;
ceo.2016.00612
D Djerić, M Folić, M Janićijević, S Blažić, D Popadić,
Recurrent malignant otitis externa with multiple
cranial nerve involvement: A case report, Srp Arh
Celok Lek. 2016 May-Jun;144(5-6):315-319
Editor's Notes
#4 They are elderly, diabetics with or without malignancy, with or without history of radiation, ķīmijterapija
#6 In diabetes mellitus, poor vascular supply resulting from microvascular disease is aggravated by pseudomonal vasculitis, which further restricts tissue perfusion. Diabetes mellitus is also associated with impaired polymorphonuclear cell function and a higher pH of cerumen in the aural canal.
#7 Dzirdes zudums – sakarā ar tūsku un pastiprinātu sekrēciju, kas aizsprosto dzirdes kanālu. Konduktīva tipa
deep otalgia persisting for longer than 1 month
Drudzis nav raksturīgs
Involvement of structures beyond the soft tissues of the auditory canal occurs only in necrotizing external otitis.
palsies generally are caused by the secretion of neurotoxins or the compressive effect of the destructive process through the relevant foramina
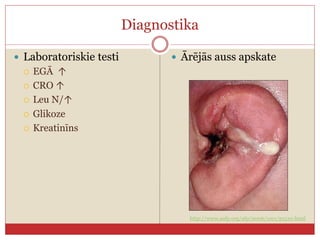
#9 Attēls - Malignant external otitis with pus draining from the necrotic ear canal and underlying osteomyelitic bone. The adjacent auricle demonstrates the swelling and loss of cartilaginous architecture characteristic of chondritis.
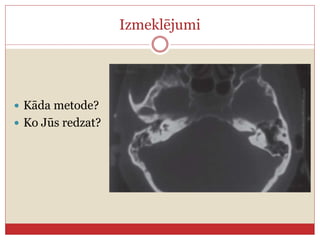
#12 CT scanning is used to determine the location and extent of diseased tissue (Figure 1). The temporal bone is the first bone to be affected, with imminent involvement of the petrous apex and mastoid. Extratemporal bone extension has become rare since the introduction of powerful antibiotics. In evaluating the CT scan, it is important to remember that at least one third of bone mineral must be lost before radiologic changes become apparent; conversely, bone remineralization continues long after the infection is cured. Thus, as related to the infectious process, pathology is late to appear on the CT scan and late to disappear. These factors limit the usefulness of CT scanning as a follow-up tool.
#13 Both osteoclasts and osteoblasts absorb 99mTc. Hence, bone scanning can locate a pathologic process in bone but is not informative about the nature of the process (infectious or other). Because the 99mTc scan remains positive as long as bone repair continues, this imaging modality is not helpful in follow-up
Attēls - Tech bone scan showed increased uptake in left temporal region
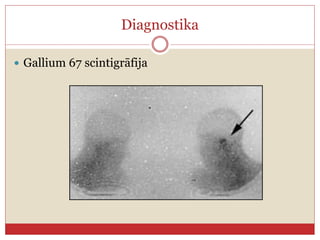
#14 Since 67Ga is absorbed by macrophages and cells of the reticuloendothelial system, scanning with this radioisotope is a sensitive measure of ongoing infectious process (Figure 2).If 67Ga scintigraphy is available, it should be used for initial diagnosis and as a follow-up tool
#17 CD – vairākus gadus, labi kontrolēta glikēmija, regulāri novērojās pie endokrinologa
#21 CT scan: Inflammatory changes involving osseous portion of external auditory canal and mastoid process
#22 Histological analysis of meatal skin, middle ear mucosa and bony septa revealed signs of chronic inflammation
and bone necrosis and calcification. The patient was discharged from the hospital after six weeks of systemic antibiotic therapy with clinical signs of recovery. During a two-month follow-up, otomicroscopy finding was normal and general condition significantly improved.
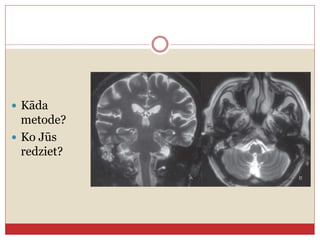
#25 CT scan and MR imaging showed devastating osteomyelitis of the petrous pyramid of the temporal bone, otomastoiditis and signs of jugular vein and lateral sinus thrombosis
MR imaging: purulent collection involving skull base (A – coronal view; B – axial view)
#26 Intensive
antibiotic therapy with vancomycin, ceftazidime, and
metronidazole combined with antimycotics gave positive
results on the condition of the patient, decreasing the
levels of inflammatory parameters after seven weeks of
treatment. Histological analysis and findings during revision
surgery of the middle ear and mastoid cavity showed
no signs of active inflammation. The patient presented
substantial postoperative recovery that was verified on CT
scan. During a six-month follow-up the patient’s hearing
improved and cranial nerves functions were completely
restored.