
Downloaded 1,148 times











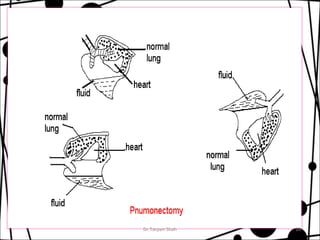


















This document discusses pulmonary surgery procedures including lobectomy, pneumonectomy, and segmental resection. It describes the indications, risks, and postoperative physiotherapy treatment for lung surgery. Key points covered are clearing lung secretions, expanding the lungs, preventing complications like infection and blood clots, regaining movement, and conditioning exercises to aid recovery.





























![Physiotherapy in pulmonary_surgery[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pulmonarysurgery1-230705093621-2b78f958-thumbnail.jpg?width=640&height=640&fit=bounds)

























































