Download as PDF, PPTX

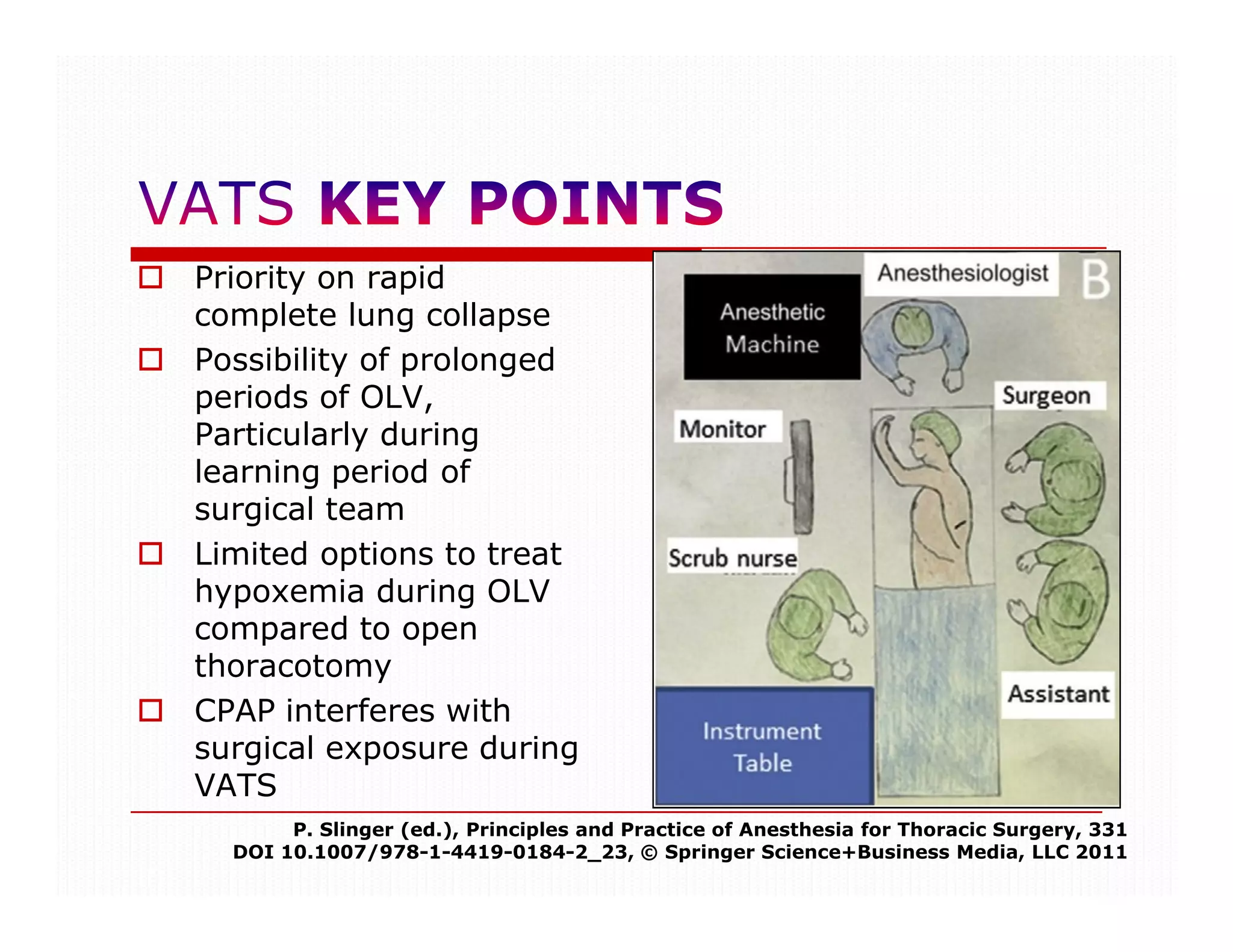





















































This document discusses considerations for one-lung ventilation (OLV) during thoracic surgery. It notes that OLV is important to rapidly collapse the lung, provide better surgical exposure, and limit options for treating hypoxemia compared to open thoracotomy. However, OLV can interfere with surgical exposure during video-assisted thoracoscopic surgery and cause delays in treating hemorrhage. The document outlines both absolute and relative indications for OLV, including isolating the surgical field from spillage and controlling ventilation distribution to prevent complications. OLV is most important for procedures involving the thoracic aorta, pneumonectomy, upper lobectomy, and mediastinal exposure.



































































