Downloaded 68 times
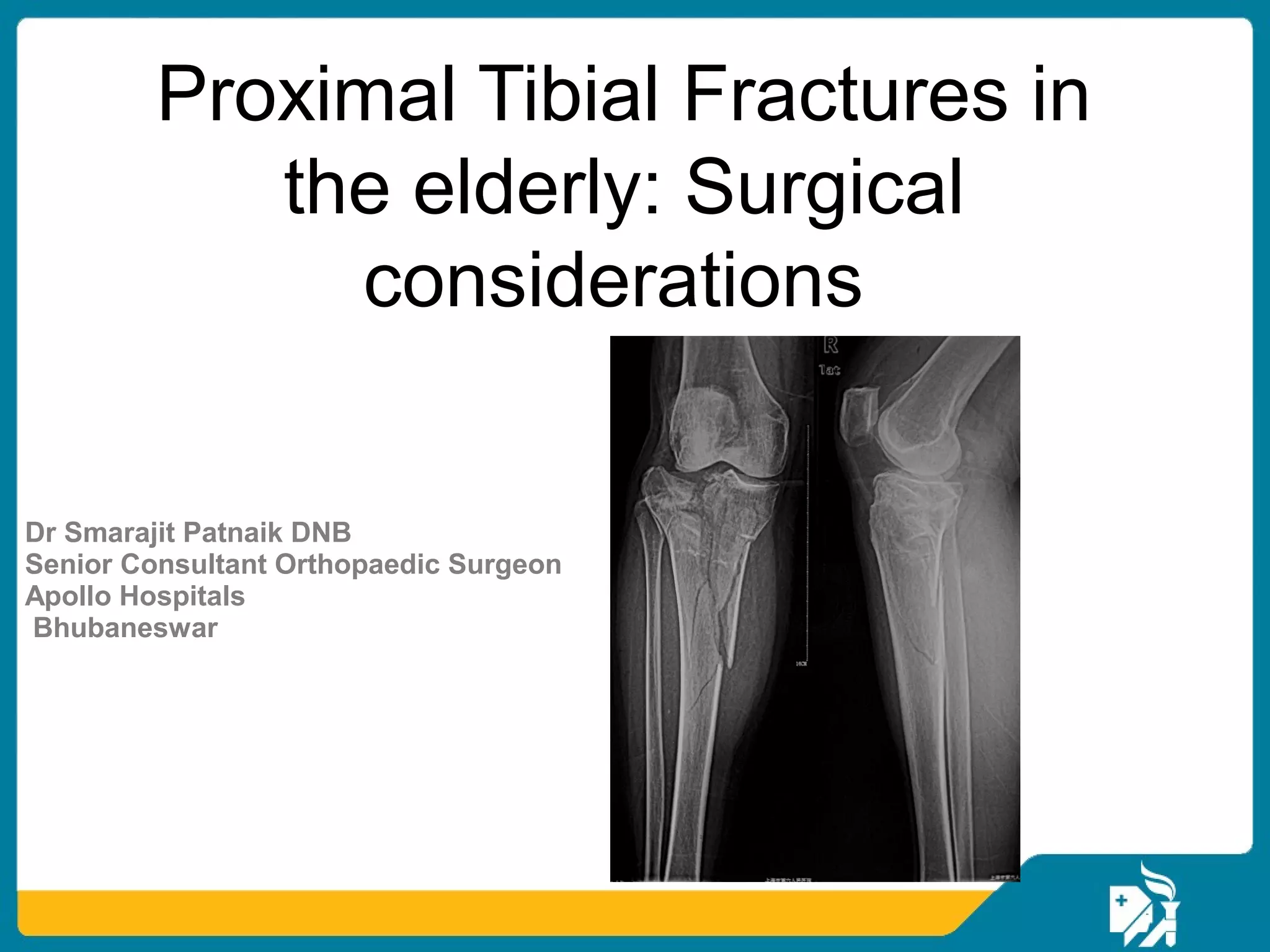

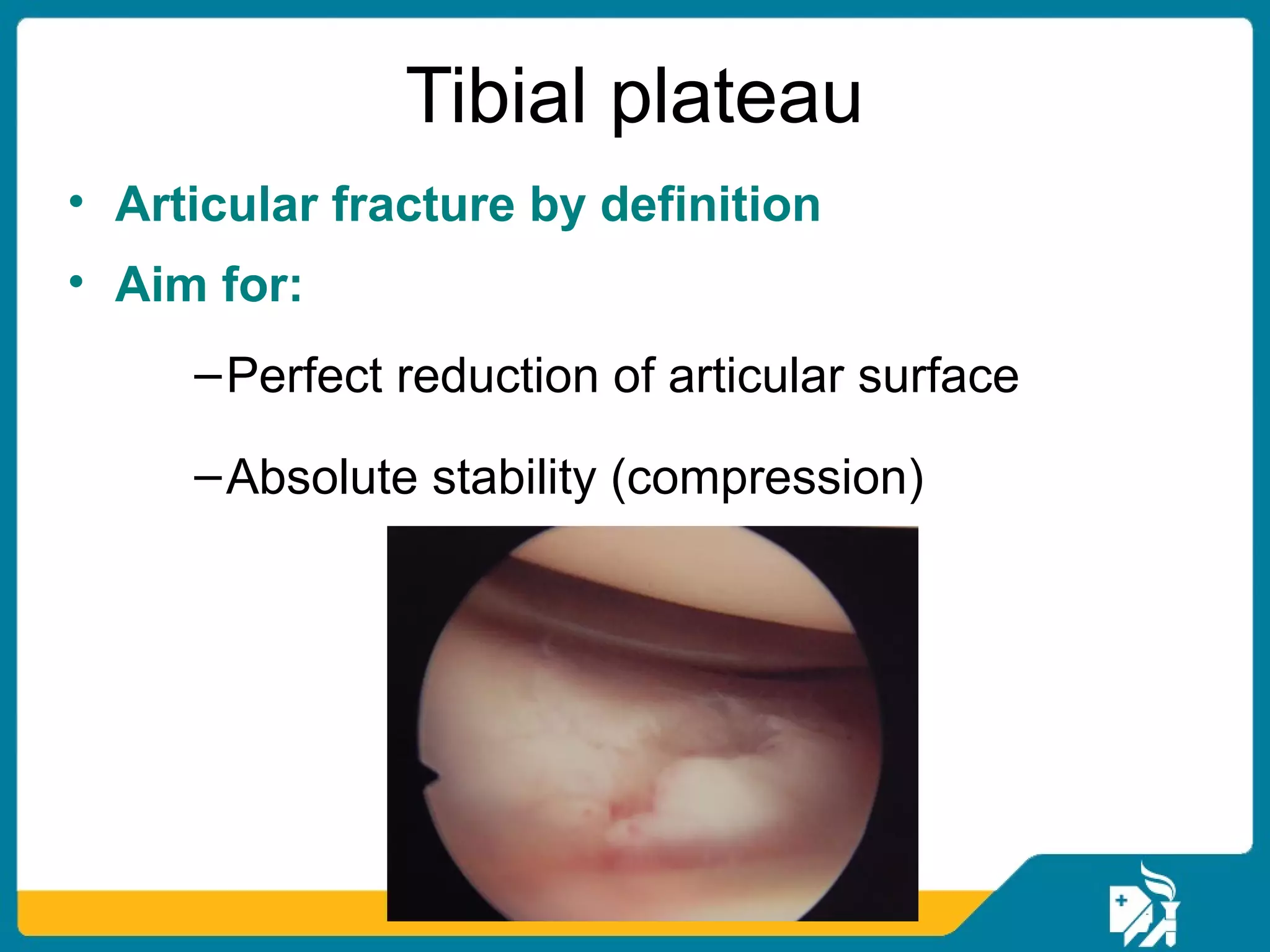
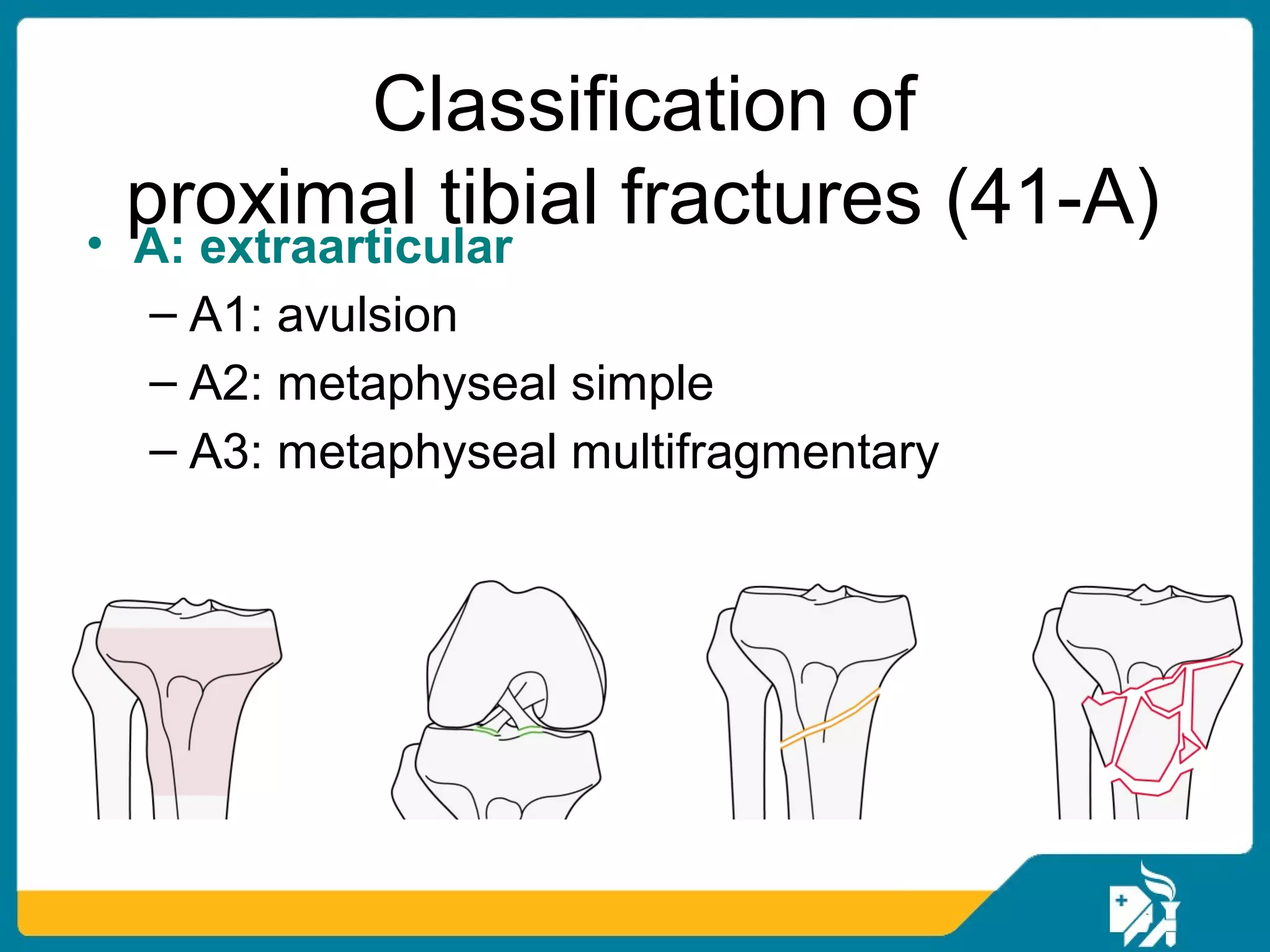
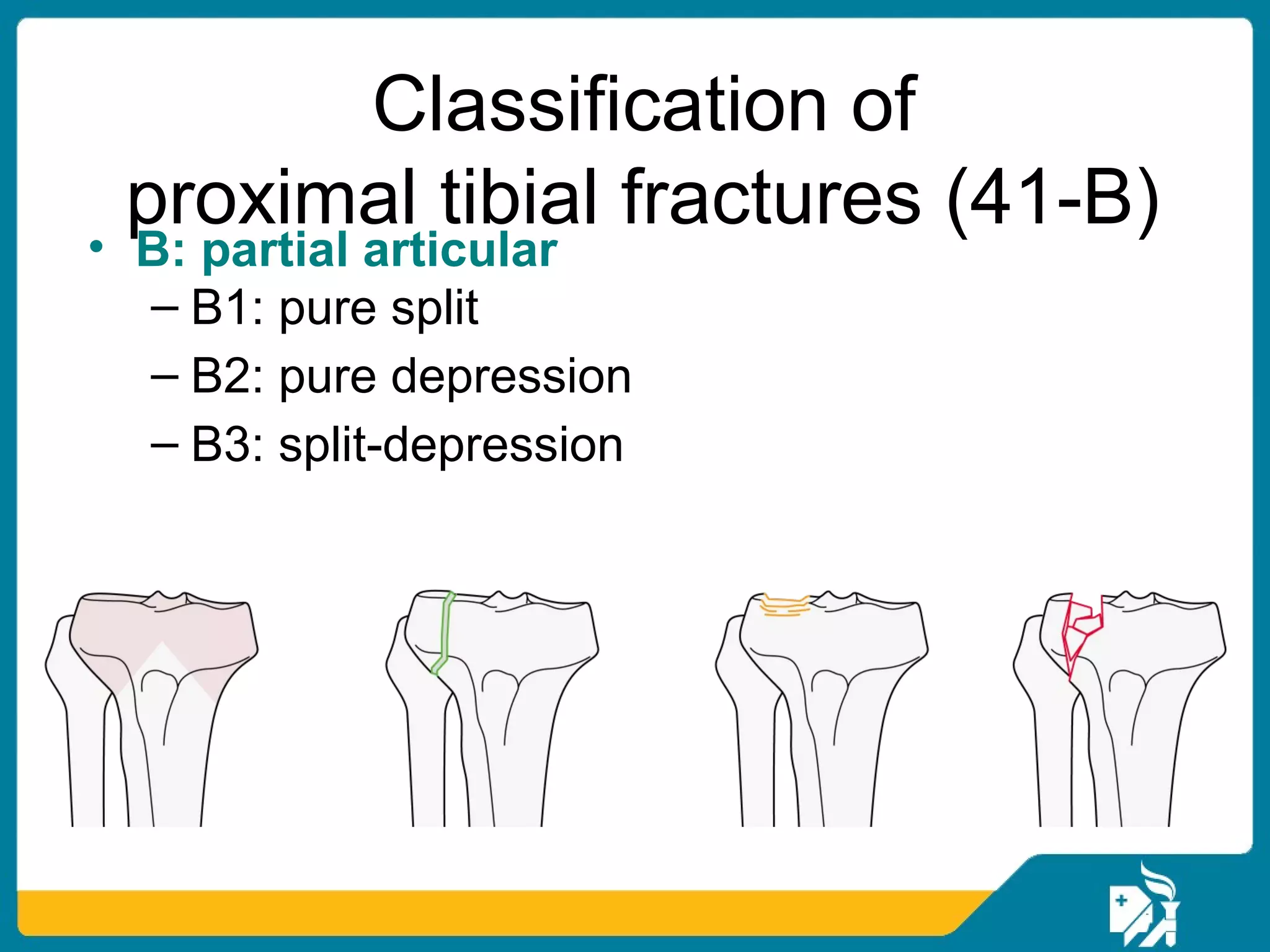
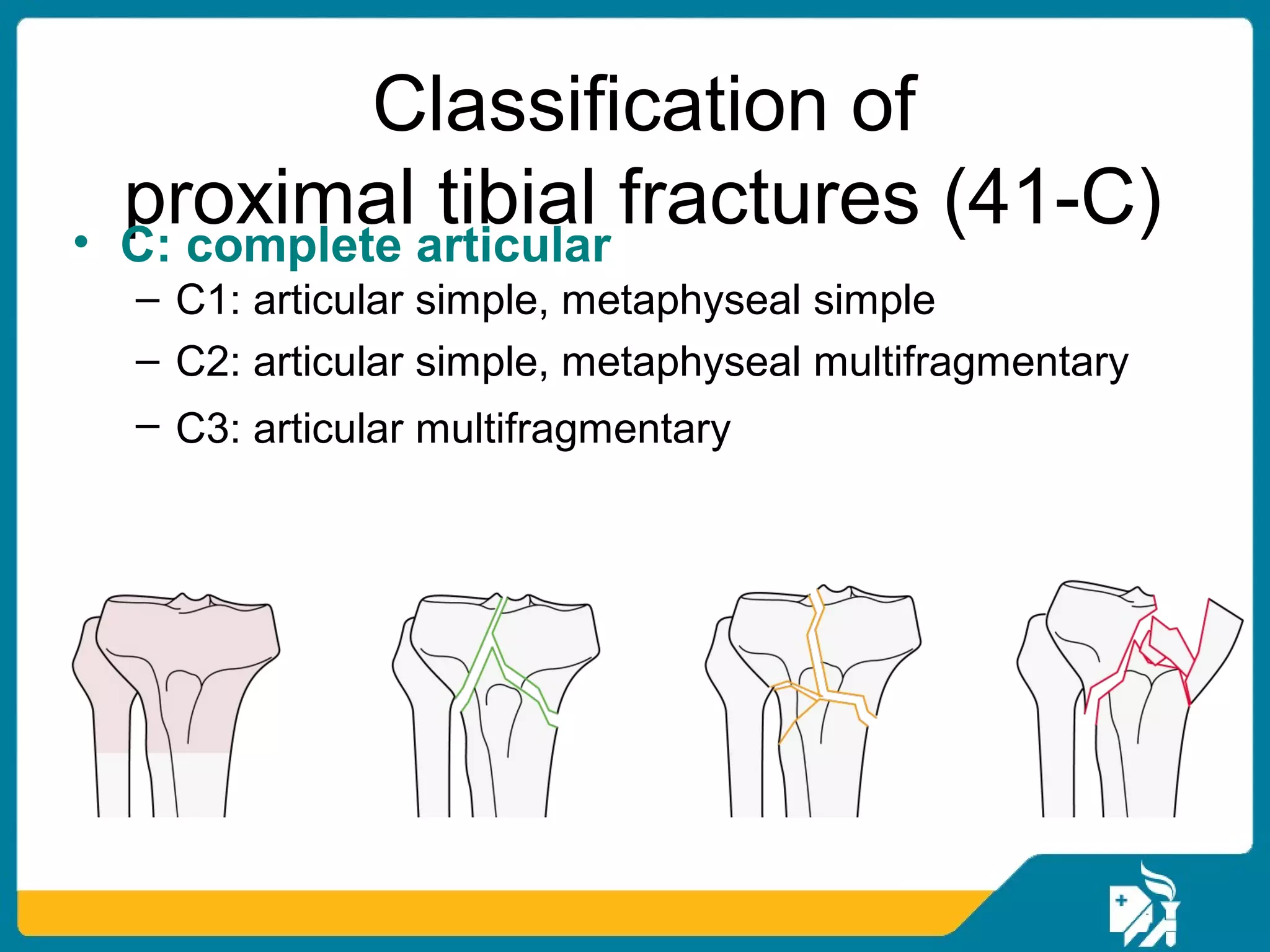

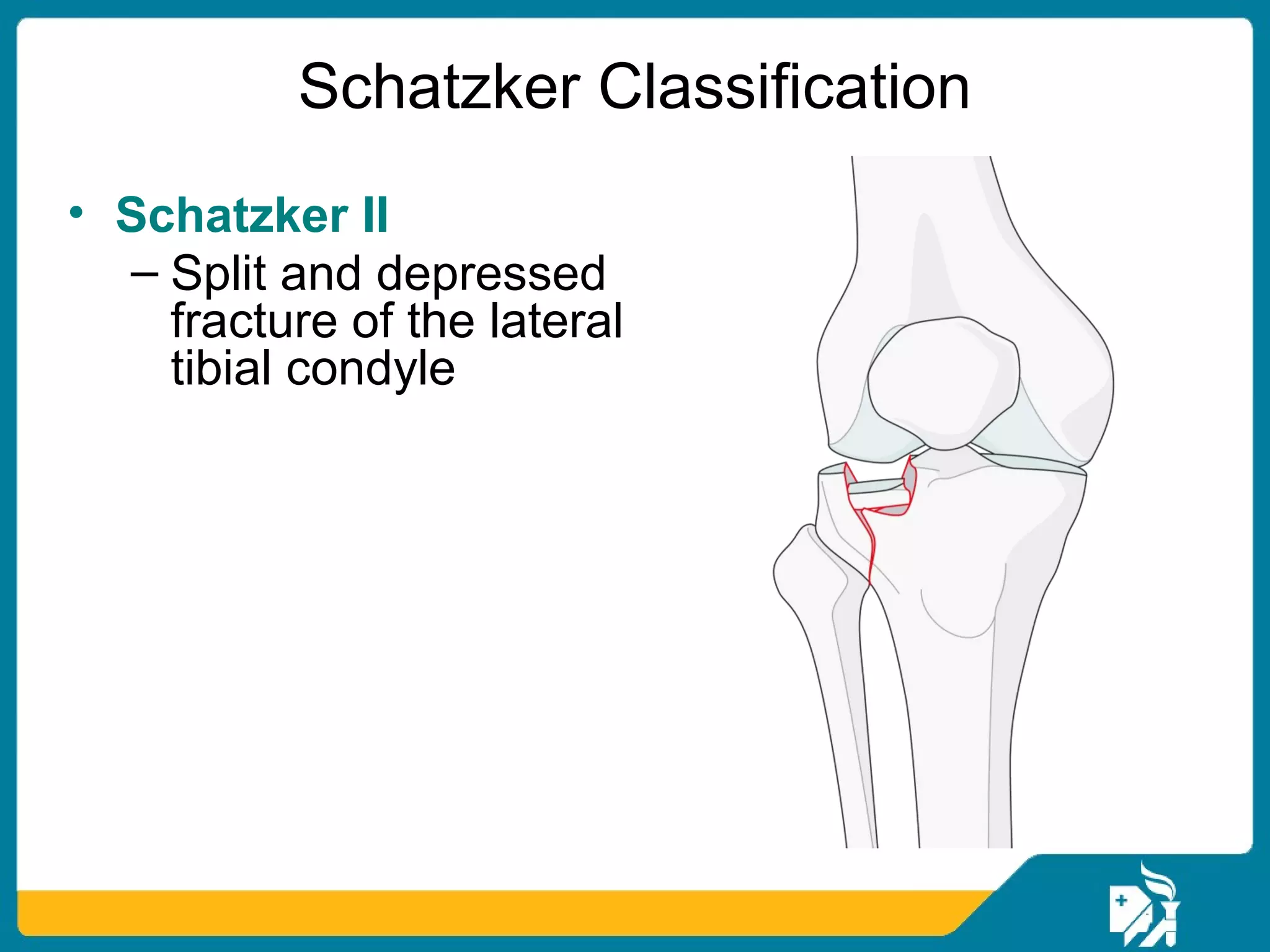
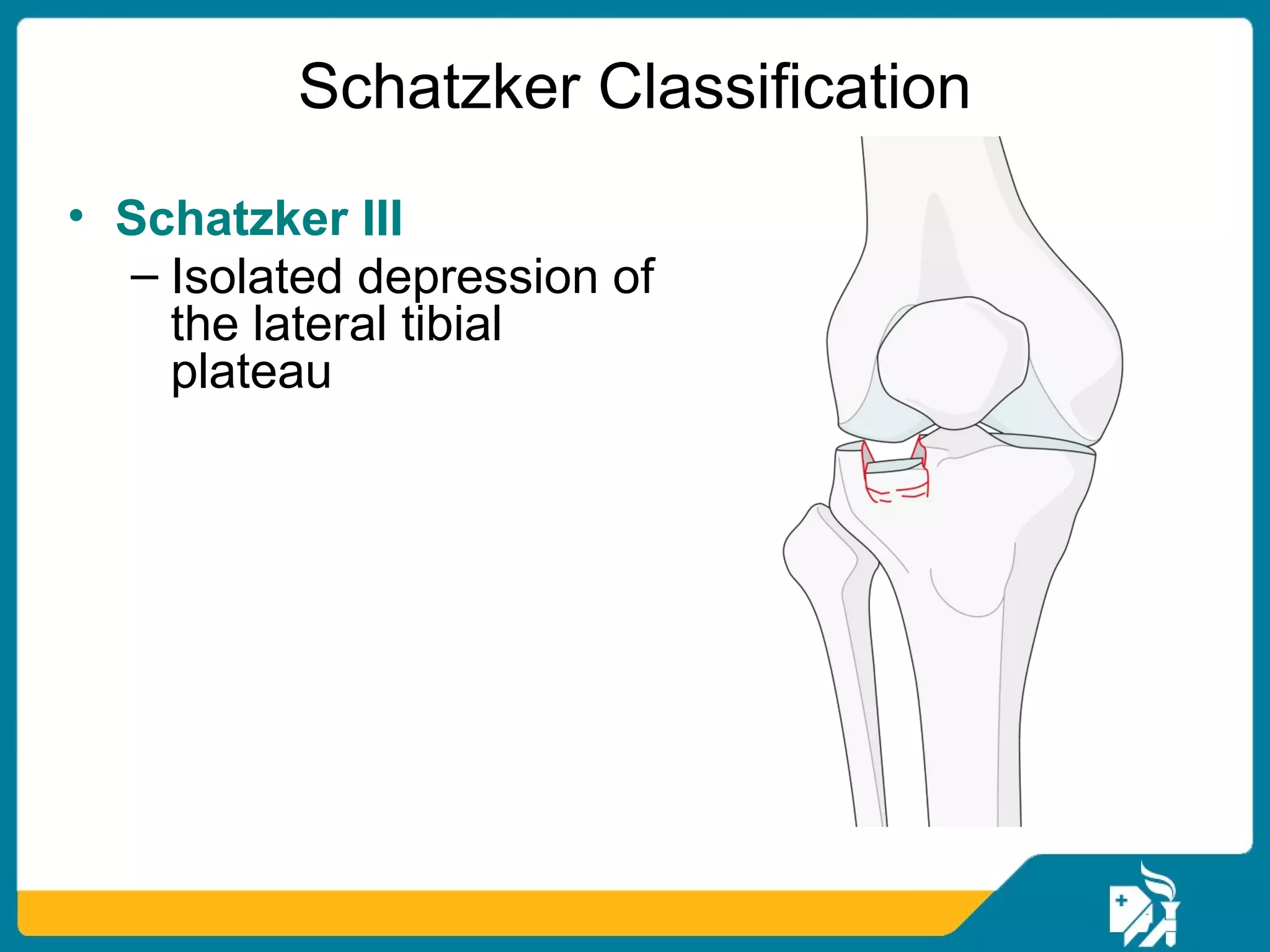
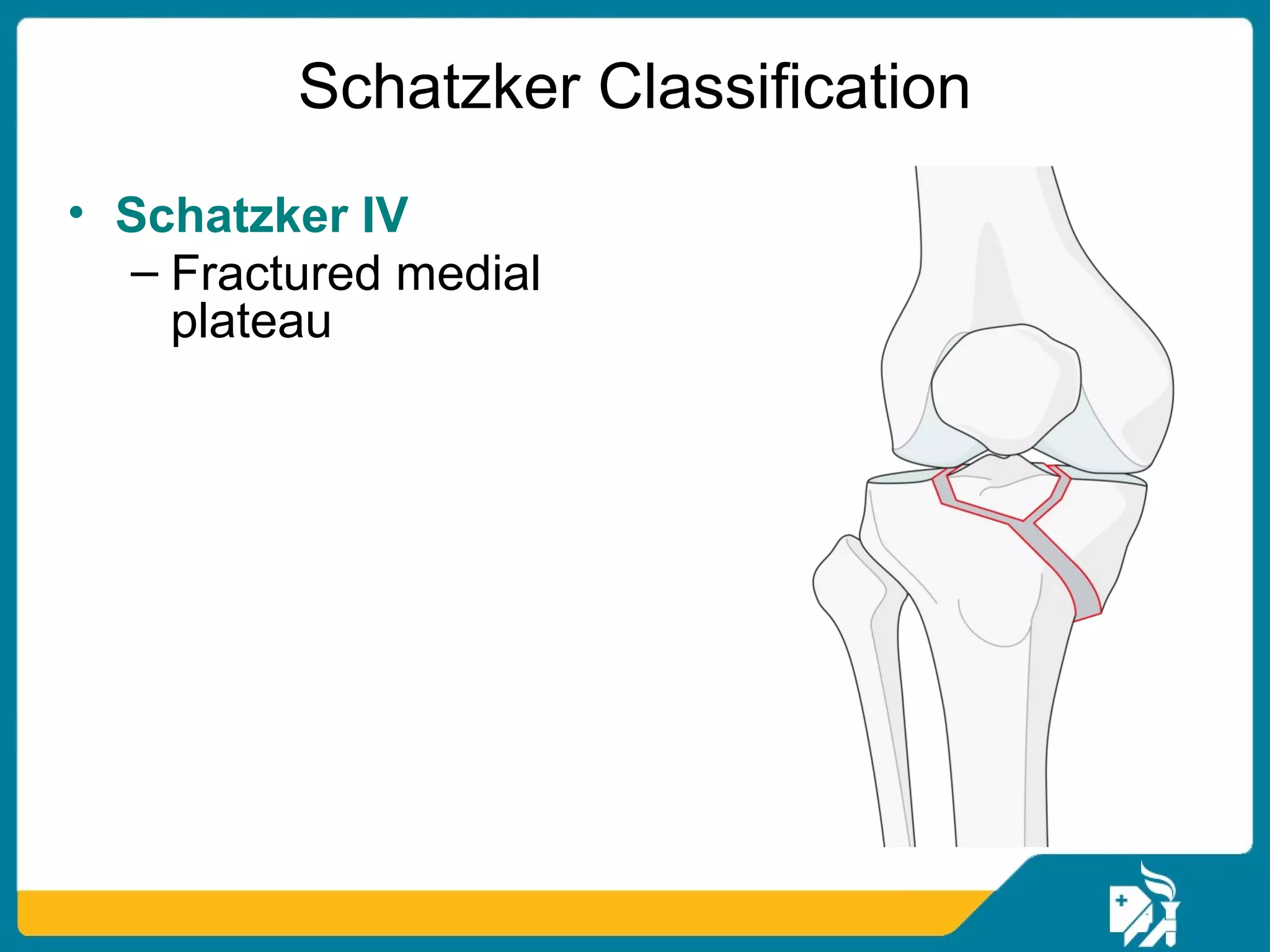
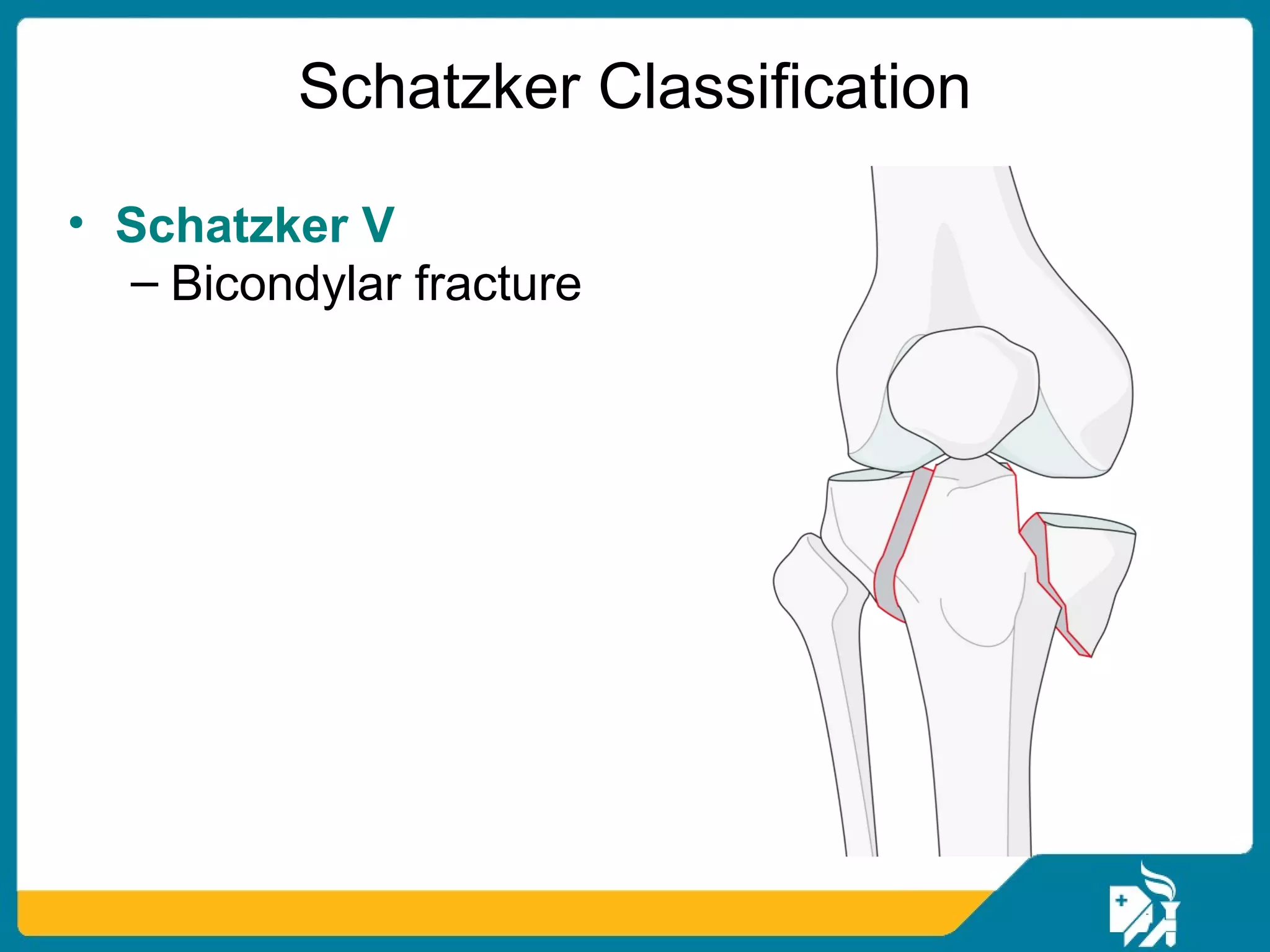
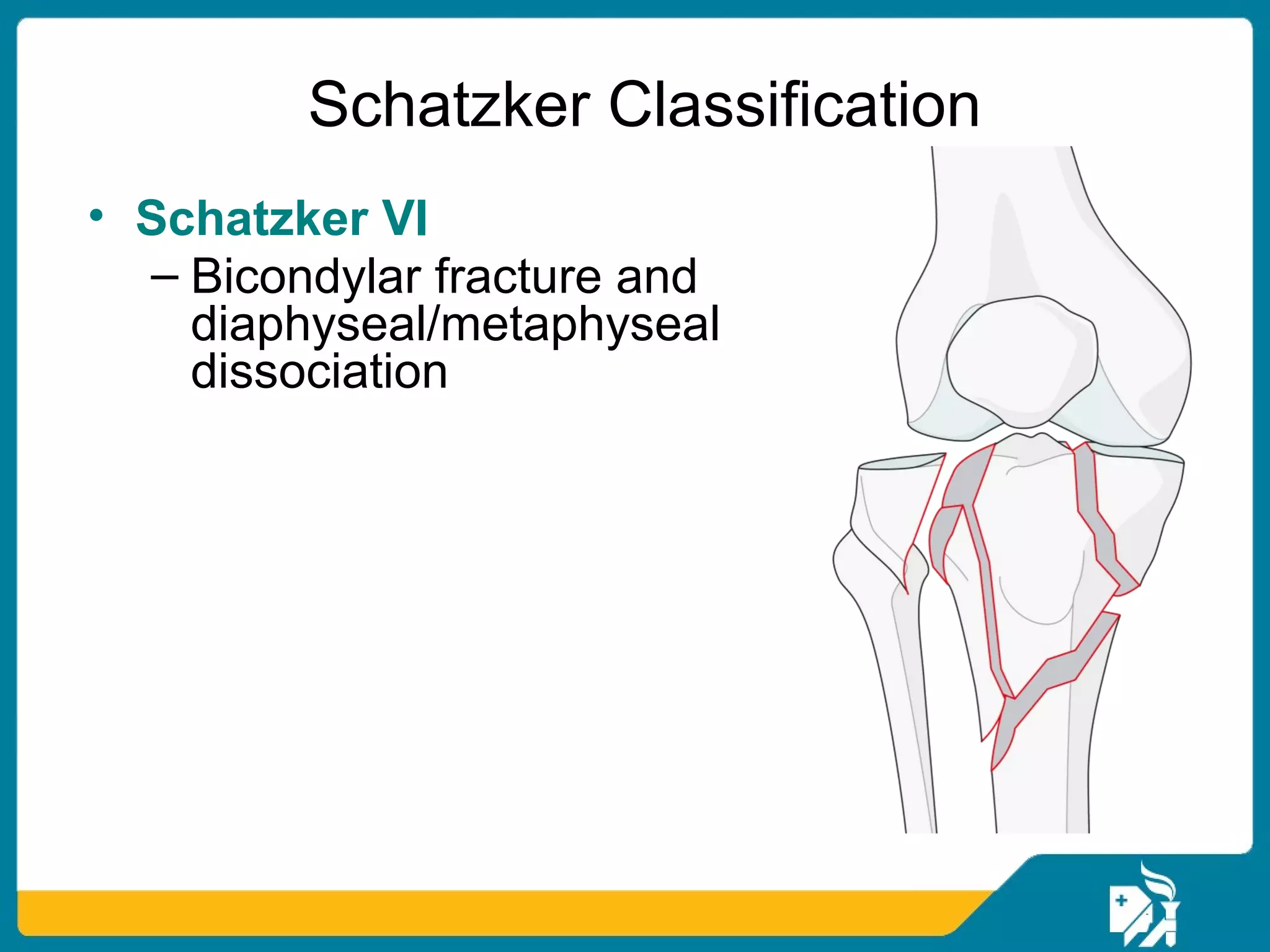




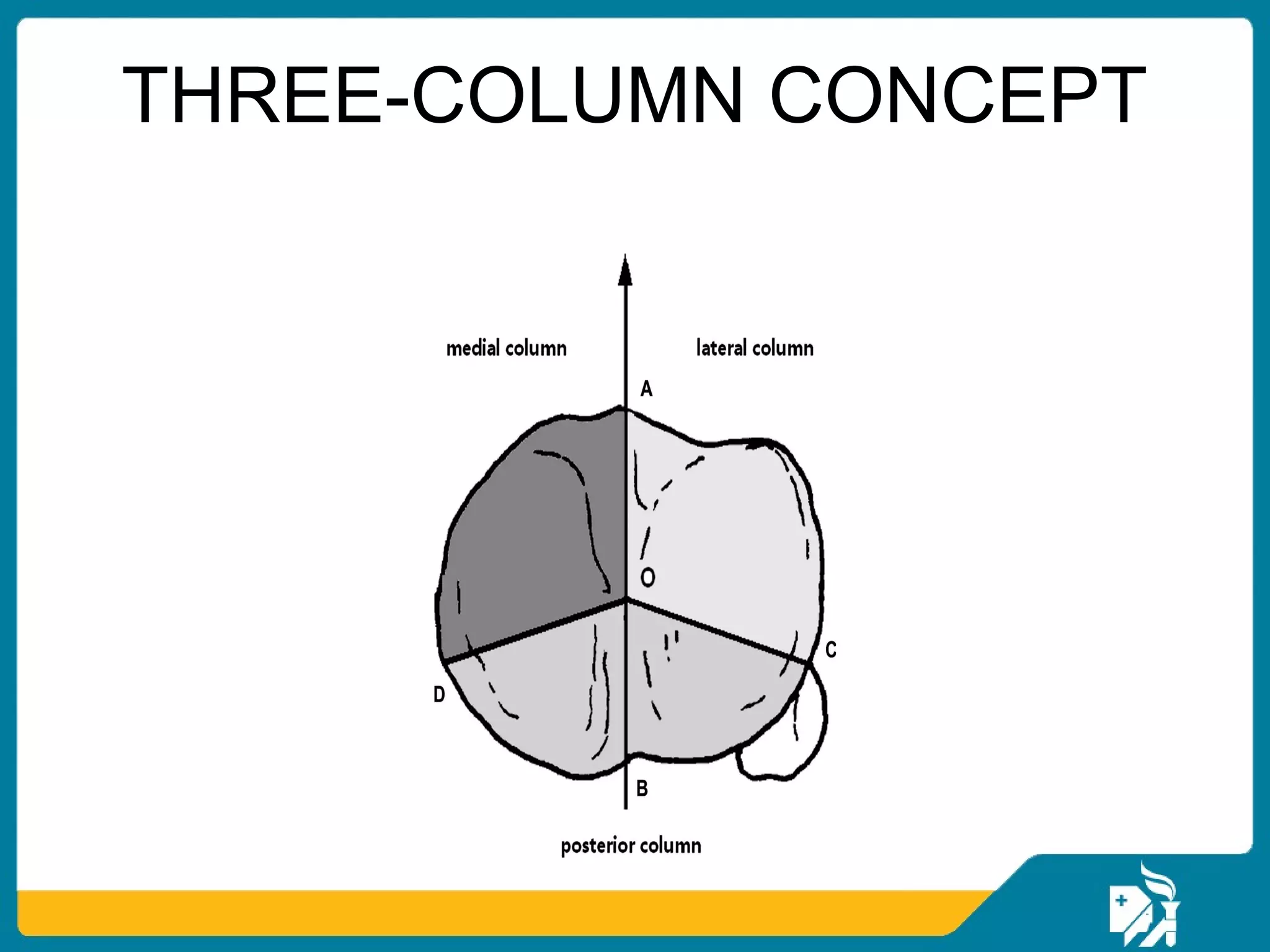
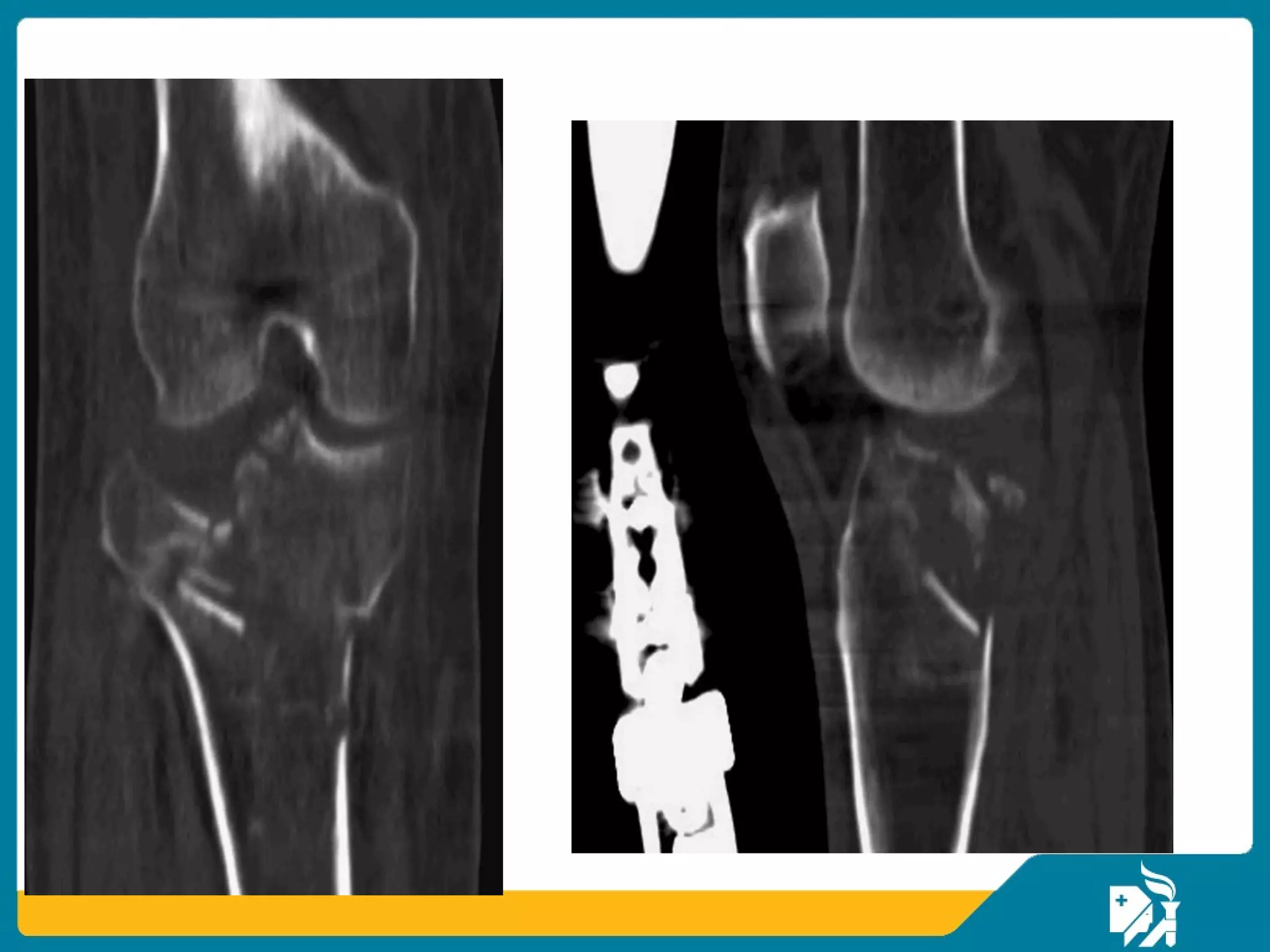









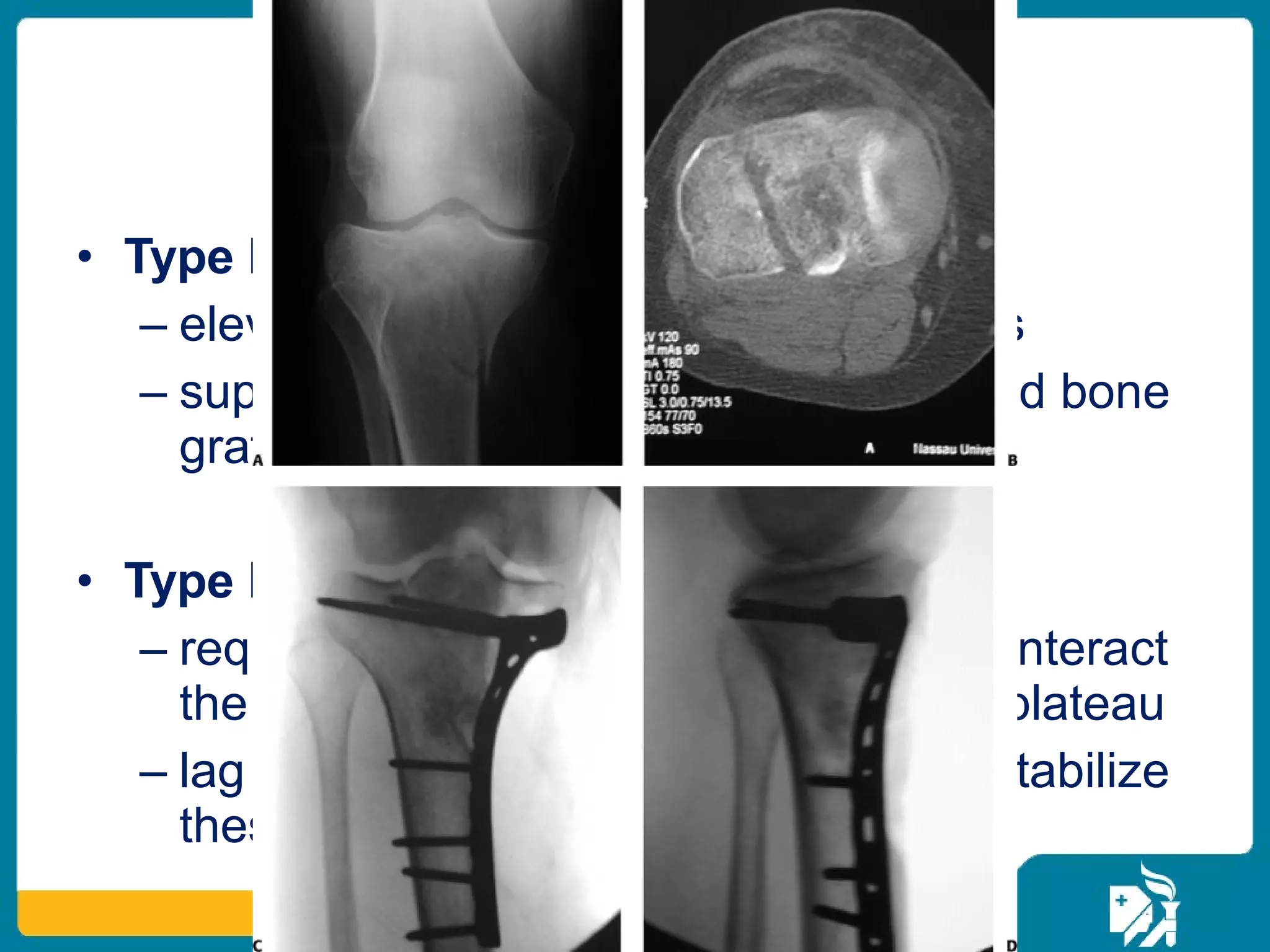

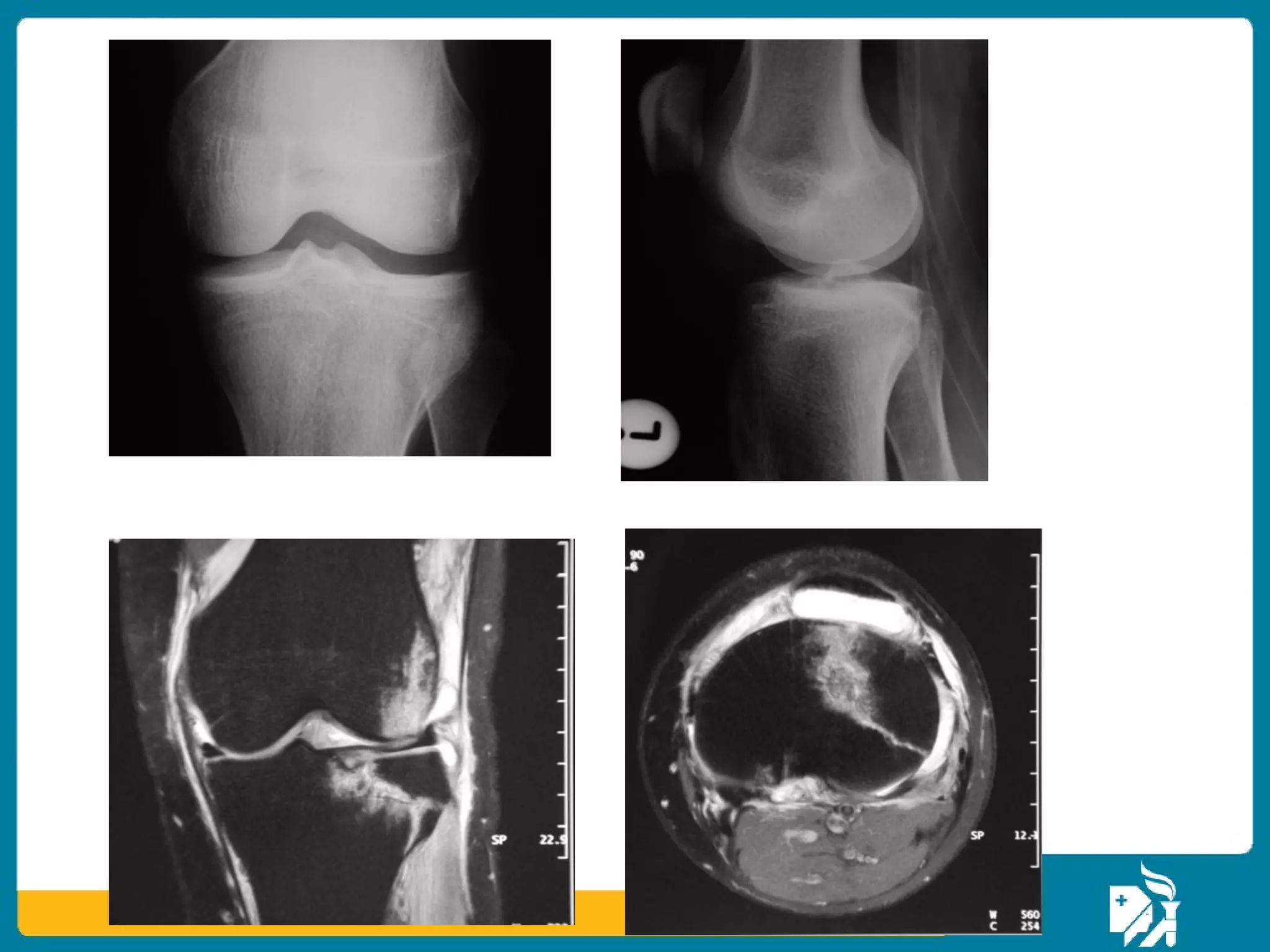



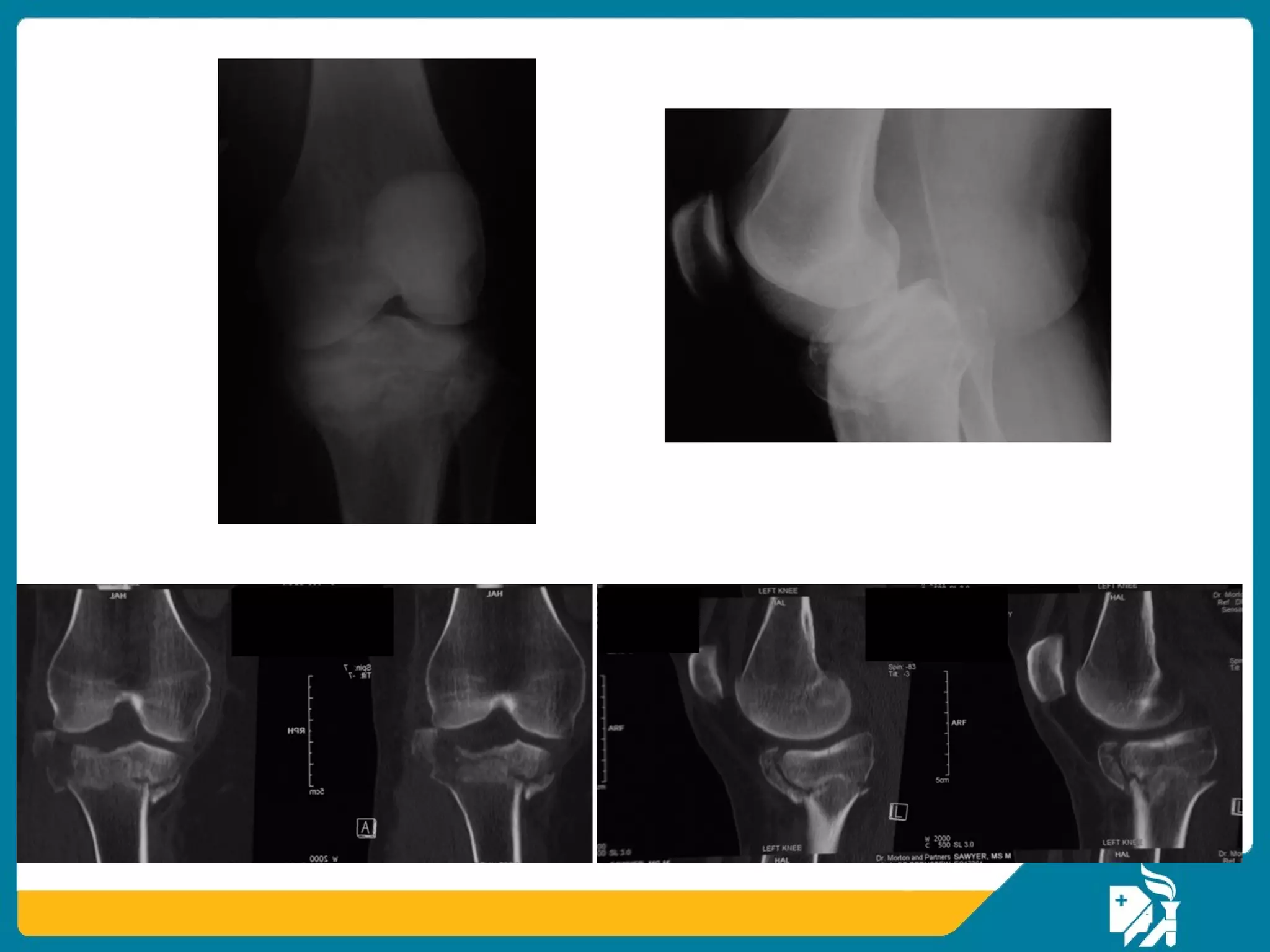
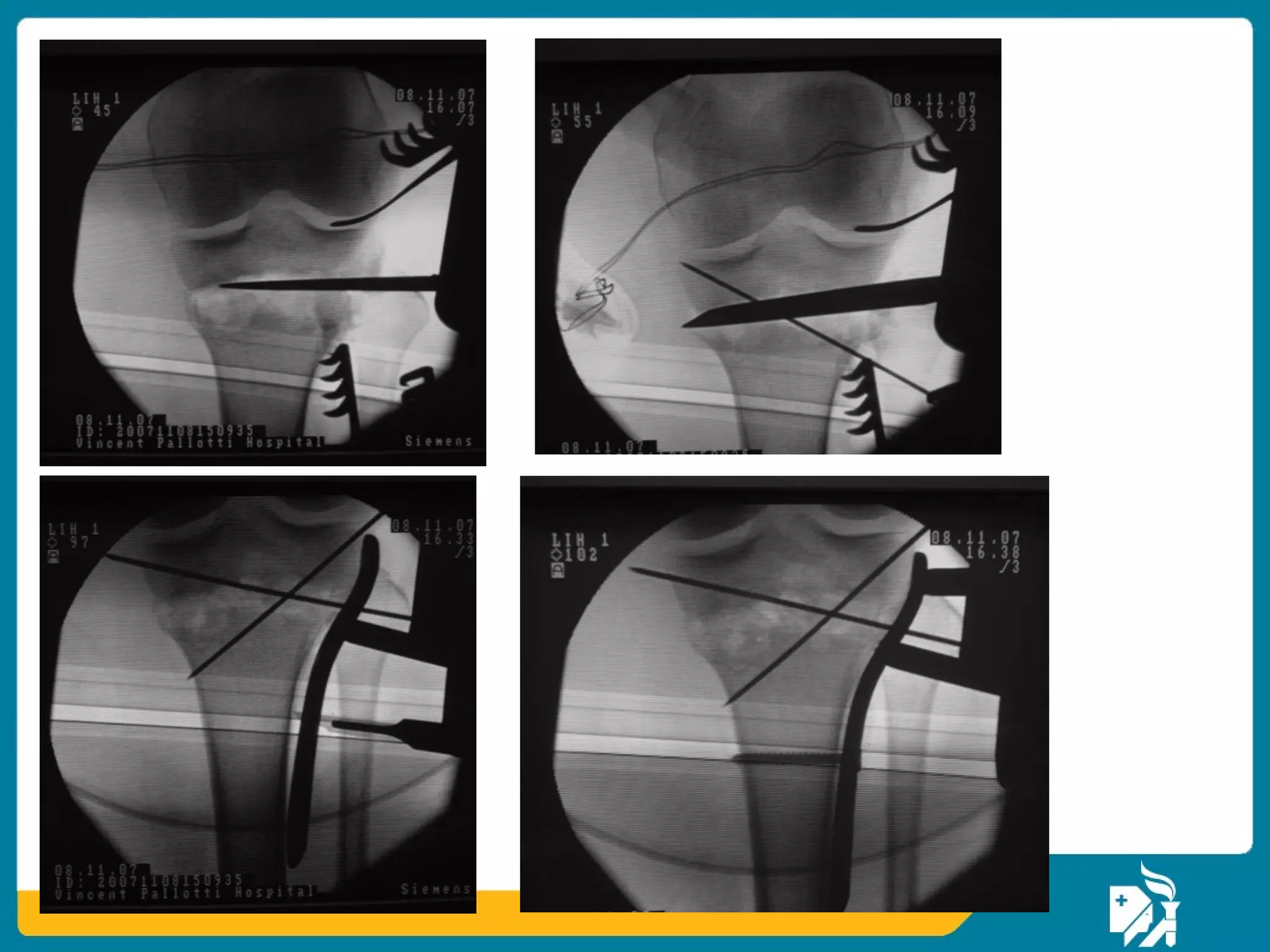

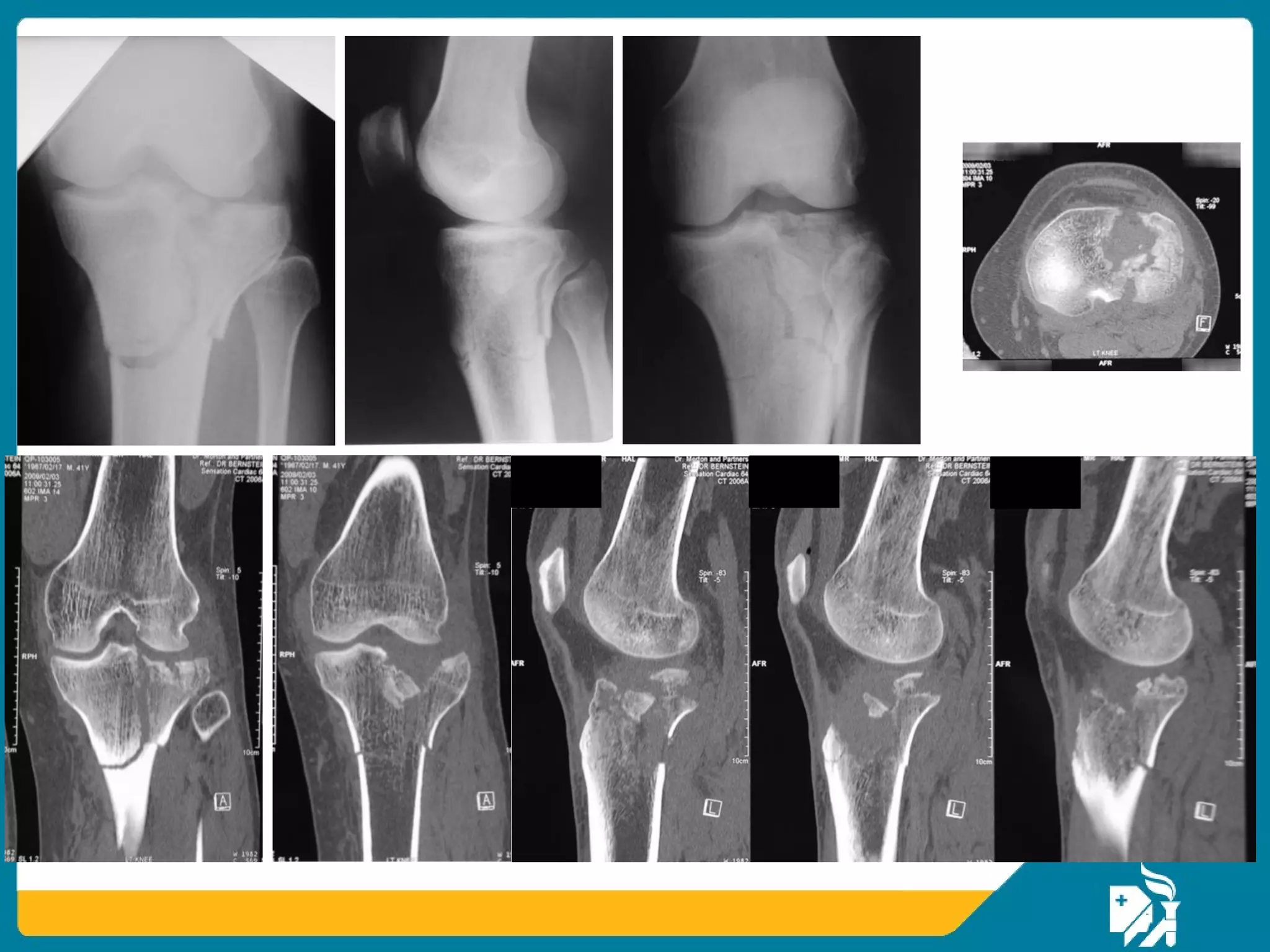













The document discusses the management of proximal tibial fractures in elderly patients, emphasizing the importance of classifying fractures and planning treatment based on their complexity. It outlines various fracture mechanisms, classifications (including Schatzker), and the necessary investigations for accurate diagnosis. The document also details surgical and non-surgical treatment options, highlighting the significance of anatomical reduction, soft tissue preservation, and early mobilization for optimal recovery outcomes.










































































