Download to read offline

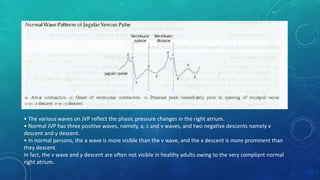


The document provides a detailed overview of jugular venous pressure (JVP), including its definition, significance, and normal wave patterns. It explains the mechanism behind the various waves in JVP and discusses abnormalities, their causes, and conditions associated with them. Additionally, it describes the hepatojugular reflux test and Kussmaul's sign, highlighting their clinical significance in diagnosing heart-related conditions.































![[Int. med] jugular venous pressure from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/ttnn2w5hsv594ygpbtvp-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171701-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)























































