Downloaded 367 times
















































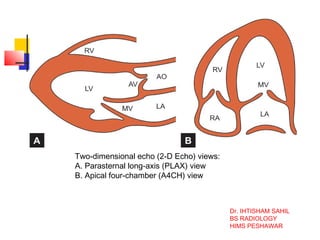











The document discusses echocardiography and stress echocardiography. It provides details on various views obtained during echocardiography including parasternal long axis, parasternal short axis, apical 4-chamber, and subcostal views. It describes the technique, advantages, and disadvantages of transthoracic echocardiography and transesophageal echocardiography. Stress echocardiography involves exercising on a treadmill or stationary bike while monitoring the heart with echocardiography before and after exercise. Dobutamine stress echocardiography uses a drug instead of exercise to stress the heart. The document is authored by Dr. Ihtisham Sahil and focuses on echocardiography techniques









































































