Downloaded 13 times

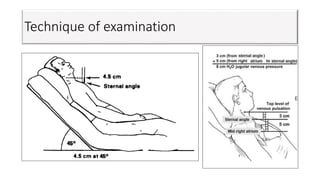

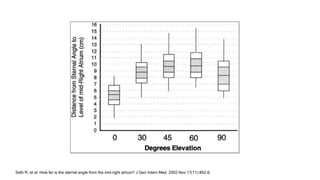
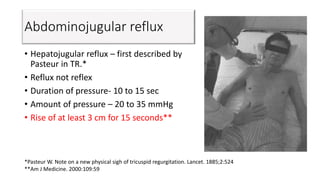
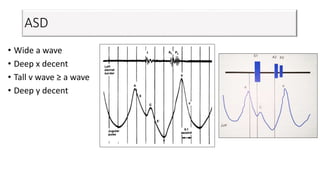

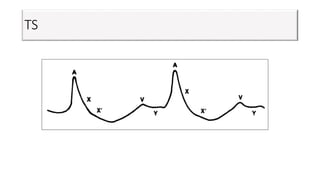
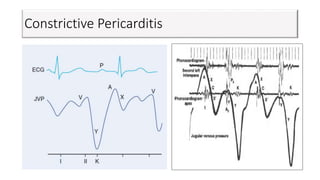
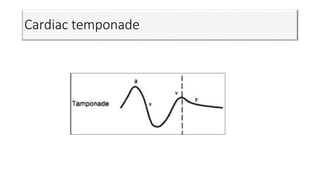
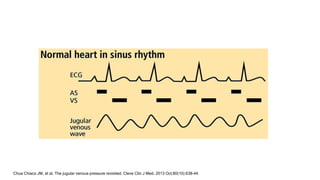
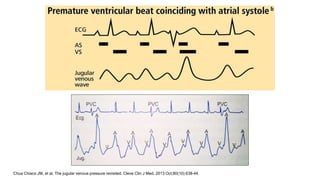
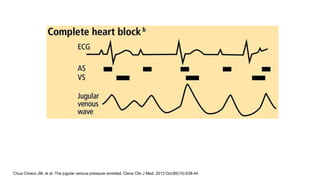
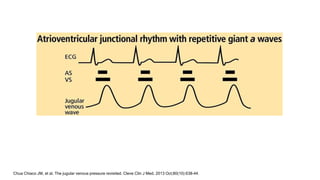


This document discusses jugular venous pressure (JVP), including: - JVP was first described in 1870 and techniques for assessment were described in 1930. - JVP reflects right atrial pressure and can provide information about cardiac function. - The internal jugular vein is best for examination. Normal JVP is less than 4 cm above the sternal angle. - Waves and pressures provide clues about conditions like tricuspid regurgitation, constrictive pericarditis, and cardiac tamponade. Proper technique is required to accurately assess JVP.




































![[Int. med] jugular venous pressure from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/ttnn2w5hsv594ygpbtvp-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171701-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)






























