Downloaded 139 times



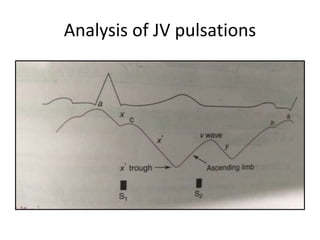
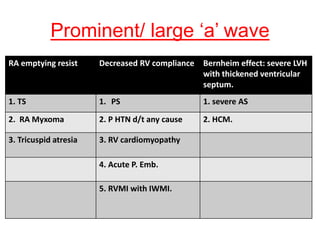
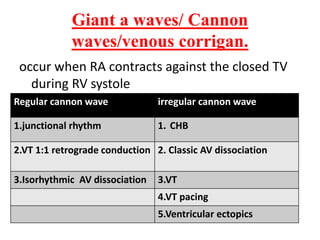
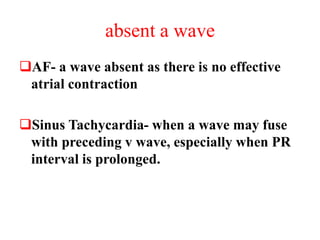
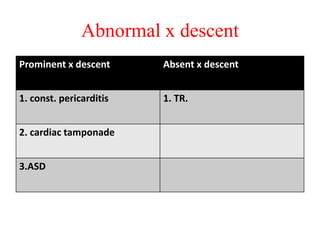
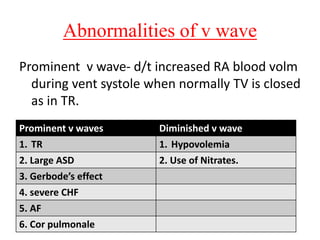
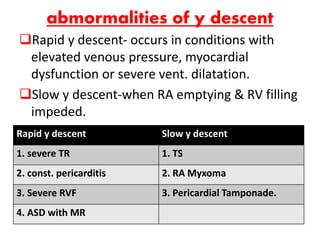
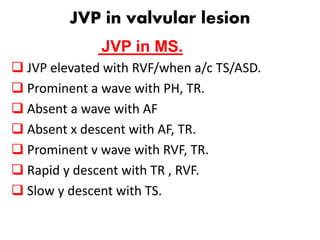
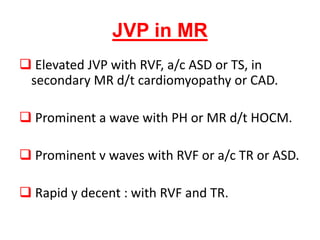

Dr. Sumedh S Ramteke's seminar discussed the jugular venous pulse (JVP) and how to assess it at the bedside. Key points included: - The JVP reflects right atrial pressure and can be used to estimate central venous pressure. - Waves include a, x, c, x', v, and y and indicate pressures in the right atrium and ventricle over the cardiac cycle. - Abnormalities in different waves provide clues about underlying conditions like tricuspid regurgitation, constrictive pericarditis, and right heart failure. - The JVP changes in characteristic ways with different arrhythmias and conduction defects. Assessment of the










































![[Int. med] jugular venous pressure from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/ttnn2w5hsv594ygpbtvp-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171701-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)






















![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






