Downloaded 28 times



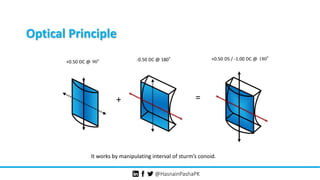



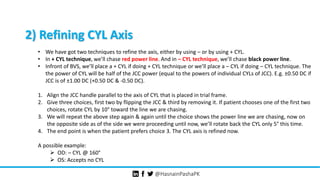
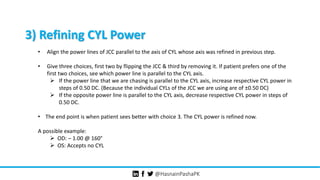




The document discusses the Jackson Cross Cylinder (JCC) technique used in clinical practice to correct astigmatism and presbyopia. It covers the history, definition, optical principles, and procedures for refining cylinder power and axis in refraction. Additionally, it details the necessary equipment and specific methods for conducting assessments effectively in patients.



































































