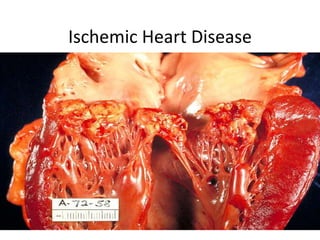
Ischemic heart disease, also known as coronary artery disease, is caused by a reduced blood supply to the heart muscle due to atherosclerosis or plaque buildup in the coronary arteries. The main symptoms include chest pain or angina on exertion. Diagnosis involves electrocardiograms, blood tests, and cardiac stress tests. Treatment focuses on controlling risk factors like high cholesterol, high blood pressure, diabetes and smoking through medications, lifestyle changes and procedures like angioplasty or bypass surgery to restore blood flow. Complications can include heart damage, heart attack and arrhythmias if not properly managed.
Acute coronary syndrome is a term used to describe a range of conditions associated with sudden, reduced blood flow to the heart.
One such condition is a heart attack (myocardial infarction) — when cell death results in damaged or destroyed heart tissue. Even when acute coronary syndrome causes no cell death, the reduced blood flow changes how your heart works and is a sign of a high risk of heart attack.
Acute coronary syndrome often causes severe chest pain or discomfort. It is a medical emergency that requires prompt diagnosis and care. The goals of treatment include improving blood flow, treating complications and preventing future problems.
Acute coronary syndrome is a term used to describe a range of conditions associated with sudden, reduced blood flow to the heart.
One such condition is a heart attack (myocardial infarction) — when cell death results in damaged or destroyed heart tissue. Even when acute coronary syndrome causes no cell death, the reduced blood flow changes how your heart works and is a sign of a high risk of heart attack.
Acute coronary syndrome often causes severe chest pain or discomfort. It is a medical emergency that requires prompt diagnosis and care. The goals of treatment include improving blood flow, treating complications and preventing future problems.
Related with cardio vascular system. Angina is Retrosternal chest pain which if left untreated can cause the higher complications with respect to cardiac health of human body. May be this is simple chest pain but if exceeds can cause major damage # prevention is better than cure :-)
Myocardial infarction is the medical name of a heart attack. A heart attack is a life-threatening condition that occurs when blood flow to the heart muscle is abruptly cut off, causing tissue damage. This is usually the result of a blockage in one or more of the coronary arteries.Symptoms include tightness or pain in the chest, neck, back or arms, as well as fatigue, lightheadedness, abnormal heartbeat and anxiety. Women are more likely to have atypical symptoms than men.
Treatment ranges from lifestyle changes and cardiac rehabilitation to medication, stents, and bypass surgery.
Prix Galien International 2024 Forum ProgramLevi Shapiro
June 20, 2024, Prix Galien International and Jerusalem Ethics Forum in ROME. Detailed agenda including panels:
- ADVANCES IN CARDIOLOGY: A NEW PARADIGM IS COMING
- WOMEN’S HEALTH: FERTILITY PRESERVATION
- WHAT’S NEW IN THE TREATMENT OF INFECTIOUS,
ONCOLOGICAL AND INFLAMMATORY SKIN DISEASES?
- ARTIFICIAL INTELLIGENCE AND ETHICS
- GENE THERAPY
- BEYOND BORDERS: GLOBAL INITIATIVES FOR DEMOCRATIZING LIFE SCIENCE TECHNOLOGIES AND PROMOTING ACCESS TO HEALTHCARE
- ETHICAL CHALLENGES IN LIFE SCIENCES
- Prix Galien International Awards Ceremony
Recomendações da OMS sobre cuidados maternos e neonatais para uma experiência pós-natal positiva.
Em consonância com os ODS – Objetivos do Desenvolvimento Sustentável e a Estratégia Global para a Saúde das Mulheres, Crianças e Adolescentes, e aplicando uma abordagem baseada nos direitos humanos, os esforços de cuidados pós-natais devem expandir-se para além da cobertura e da simples sobrevivência, de modo a incluir cuidados de qualidade.
Estas diretrizes visam melhorar a qualidade dos cuidados pós-natais essenciais e de rotina prestados às mulheres e aos recém-nascidos, com o objetivo final de melhorar a saúde e o bem-estar materno e neonatal.
Uma “experiência pós-natal positiva” é um resultado importante para todas as mulheres que dão à luz e para os seus recém-nascidos, estabelecendo as bases para a melhoria da saúde e do bem-estar a curto e longo prazo. Uma experiência pós-natal positiva é definida como aquela em que as mulheres, pessoas que gestam, os recém-nascidos, os casais, os pais, os cuidadores e as famílias recebem informação consistente, garantia e apoio de profissionais de saúde motivados; e onde um sistema de saúde flexível e com recursos reconheça as necessidades das mulheres e dos bebês e respeite o seu contexto cultural.
Estas diretrizes consolidadas apresentam algumas recomendações novas e já bem fundamentadas sobre cuidados pós-natais de rotina para mulheres e neonatos que recebem cuidados no pós-parto em unidades de saúde ou na comunidade, independentemente dos recursos disponíveis.
É fornecido um conjunto abrangente de recomendações para cuidados durante o período puerperal, com ênfase nos cuidados essenciais que todas as mulheres e recém-nascidos devem receber, e com a devida atenção à qualidade dos cuidados; isto é, a entrega e a experiência do cuidado recebido. Estas diretrizes atualizam e ampliam as recomendações da OMS de 2014 sobre cuidados pós-natais da mãe e do recém-nascido e complementam as atuais diretrizes da OMS sobre a gestão de complicações pós-natais.
O estabelecimento da amamentação e o manejo das principais intercorrências é contemplada.
Recomendamos muito.
Vamos discutir essas recomendações no nosso curso de pós-graduação em Aleitamento no Instituto Ciclos.
Esta publicação só está disponível em inglês até o momento.
Prof. Marcus Renato de Carvalho
www.agostodourado.com
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?bkling
Are you curious about what’s new in cervical cancer research or unsure what the findings mean? Join Dr. Emily Ko, a gynecologic oncologist at Penn Medicine, to learn about the latest updates from the Society of Gynecologic Oncology (SGO) 2024 Annual Meeting on Women’s Cancer. Dr. Ko will discuss what the research presented at the conference means for you and answer your questions about the new developments.
These simplified slides by Dr. Sidra Arshad present an overview of the non-respiratory functions of the respiratory tract.
Learning objectives:
1. Enlist the non-respiratory functions of the respiratory tract
2. Briefly explain how these functions are carried out
3. Discuss the significance of dead space
4. Differentiate between minute ventilation and alveolar ventilation
5. Describe the cough and sneeze reflexes
Study Resources:
1. Chapter 39, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 34, Ganong’s Review of Medical Physiology, 26th edition
3. Chapter 17, Human Physiology by Lauralee Sherwood, 9th edition
4. Non-respiratory functions of the lungs https://academic.oup.com/bjaed/article/13/3/98/278874
Title: Sense of Taste
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the structure and function of taste buds.
Describe the relationship between the taste threshold and taste index of common substances.
Explain the chemical basis and signal transduction of taste perception for each type of primary taste sensation.
Recognize different abnormalities of taste perception and their causes.
Key Topics:
Significance of Taste Sensation:
Differentiation between pleasant and harmful food
Influence on behavior
Selection of food based on metabolic needs
Receptors of Taste:
Taste buds on the tongue
Influence of sense of smell, texture of food, and pain stimulation (e.g., by pepper)
Primary and Secondary Taste Sensations:
Primary taste sensations: Sweet, Sour, Salty, Bitter, Umami
Chemical basis and signal transduction mechanisms for each taste
Taste Threshold and Index:
Taste threshold values for Sweet (sucrose), Salty (NaCl), Sour (HCl), and Bitter (Quinine)
Taste index relationship: Inversely proportional to taste threshold
Taste Blindness:
Inability to taste certain substances, particularly thiourea compounds
Example: Phenylthiocarbamide
Structure and Function of Taste Buds:
Composition: Epithelial cells, Sustentacular/Supporting cells, Taste cells, Basal cells
Features: Taste pores, Taste hairs/microvilli, and Taste nerve fibers
Location of Taste Buds:
Found in papillae of the tongue (Fungiform, Circumvallate, Foliate)
Also present on the palate, tonsillar pillars, epiglottis, and proximal esophagus
Mechanism of Taste Stimulation:
Interaction of taste substances with receptors on microvilli
Signal transduction pathways for Umami, Sweet, Bitter, Sour, and Salty tastes
Taste Sensitivity and Adaptation:
Decrease in sensitivity with age
Rapid adaptation of taste sensation
Role of Saliva in Taste:
Dissolution of tastants to reach receptors
Washing away the stimulus
Taste Preferences and Aversions:
Mechanisms behind taste preference and aversion
Influence of receptors and neural pathways
Impact of Sensory Nerve Damage:
Degeneration of taste buds if the sensory nerve fiber is cut
Abnormalities of Taste Detection:
Conditions: Ageusia, Hypogeusia, Dysgeusia (parageusia)
Causes: Nerve damage, neurological disorders, infections, poor oral hygiene, adverse drug effects, deficiencies, aging, tobacco use, altered neurotransmitter levels
Neurotransmitters and Taste Threshold:
Effects of serotonin (5-HT) and norepinephrine (NE) on taste sensitivity
Supertasters:
25% of the population with heightened sensitivity to taste, especially bitterness
Increased number of fungiform papillae
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...i3 Health
i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource.
This slide deck presented by Dr. Kami Maddocks, Professor-Clinical in the Division of Hematology and
Associate Division Director for Ambulatory Operations
The Ohio State University Comprehensive Cancer Center, will provide insight into new directions in targeted therapeutic approaches for older adults with mantle cell lymphoma.
STATEMENT OF NEED
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma (NHL) accounting for 5% to 7% of all lymphomas. Its prognosis ranges from indolent disease that does not require treatment for years to very aggressive disease, which is associated with poor survival (Silkenstedt et al, 2021). Typically, MCL is diagnosed at advanced stage and in older patients who cannot tolerate intensive therapy (NCCN, 2022). Although recent advances have slightly increased remission rates, recurrence and relapse remain very common, leading to a median overall survival between 3 and 6 years (LLS, 2021). Though there are several effective options, progress is still needed towards establishing an accepted frontline approach for MCL (Castellino et al, 2022). Treatment selection and management of MCL are complicated by the heterogeneity of prognosis, advanced age and comorbidities of patients, and lack of an established standard approach for treatment, making it vital that clinicians be familiar with the latest research and advances in this area. In this activity chaired by Michael Wang, MD, Professor in the Department of Lymphoma & Myeloma at MD Anderson Cancer Center, expert faculty will discuss prognostic factors informing treatment, the promising results of recent trials in new therapeutic approaches, and the implications of treatment resistance in therapeutic selection for MCL.
Target Audience
Hematology/oncology fellows, attending faculty, and other health care professionals involved in the treatment of patients with mantle cell lymphoma (MCL).
Learning Objectives
1.) Identify clinical and biological prognostic factors that can guide treatment decision making for older adults with MCL
2.) Evaluate emerging data on targeted therapeutic approaches for treatment-naive and relapsed/refractory MCL and their applicability to older adults
3.) Assess mechanisms of resistance to targeted therapies for MCL and their implications for treatment selection
Ethanol (CH3CH2OH), or beverage alcohol, is a two-carbon alcohol
that is rapidly distributed in the body and brain. Ethanol alters many
neurochemical systems and has rewarding and addictive properties. It
is the oldest recreational drug and likely contributes to more morbidity,
mortality, and public health costs than all illicit drugs combined. The
5th edition of the Diagnostic and Statistical Manual of Mental Disorders
(DSM-5) integrates alcohol abuse and alcohol dependence into a single
disorder called alcohol use disorder (AUD), with mild, moderate,
and severe subclassifications (American Psychiatric Association, 2013).
In the DSM-5, all types of substance abuse and dependence have been
combined into a single substance use disorder (SUD) on a continuum
from mild to severe. A diagnosis of AUD requires that at least two of
the 11 DSM-5 behaviors be present within a 12-month period (mild
AUD: 2–3 criteria; moderate AUD: 4–5 criteria; severe AUD: 6–11 criteria).
The four main behavioral effects of AUD are impaired control over
drinking, negative social consequences, risky use, and altered physiological
effects (tolerance, withdrawal). This chapter presents an overview
of the prevalence and harmful consequences of AUD in the U.S.,
the systemic nature of the disease, neurocircuitry and stages of AUD,
comorbidities, fetal alcohol spectrum disorders, genetic risk factors, and
pharmacotherapies for AUD.
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...Oleg Kshivets
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
NVBDCP.pptx Nation vector borne disease control programSapna Thakur
NVBDCP was launched in 2003-2004 . Vector-Borne Disease: Disease that results from an infection transmitted to humans and other animals by blood-feeding arthropods, such as mosquitoes, ticks, and fleas. Examples of vector-borne diseases include Dengue fever, West Nile Virus, Lyme disease, and malaria.
ARTIFICIAL INTELLIGENCE IN HEALTHCARE.pdfAnujkumaranit
Artificial intelligence (AI) refers to the simulation of human intelligence processes by machines, especially computer systems. It encompasses tasks such as learning, reasoning, problem-solving, perception, and language understanding. AI technologies are revolutionizing various fields, from healthcare to finance, by enabling machines to perform tasks that typically require human intelligence.
2. Definition
• (IHD), myocardial ischemia or
CAD(coronary heart disease)is a
disease characterized by ischemia
(reduced blood supply) to the heart
muscle,
usually due to coronary artery disease
(atherosclerosis of the coronary
arteries obstruction )
3. • Imbalance between Myocardial
oxygen supply and demand.
• Myocardial hypoxia and
accumulation of waste metabolites
due to atherosclerotic disease of
coronary arteries
• Most occurs because of
atherosclerotic plaque with in one or
more coronary arteries
5. Etiology and Pathophsiology
• The disease process underlying
most ischemic heart disease is
atherosclerosis of the coronary
arteries.
• The arteries become "furred up"
by fat-rich deposits in the vessel
wall (plaques).
6. Epidmiology
• IHD Is the number one killer in USA and
worldwide
• Every minute an American dies of CAD
• 37% who experience acute coronary
syndrome will die of it in the same year
• Since 1968 CAD decreased annually –from
1980 to 2000 CAD reduced to half proper
treatment and improved risk factors
• Still 1/6 death is due CAD
• Still CAD affecting 16 million American
• CAD increased by age
7. Angina pectoris
• Is the most common cardiac pain, it is usually
due to myocardial ischemia from obstructed
flow in coronary vessels .
But can occur by other conditions
• Aortic stenosis
• Hypertrophy
• Cardiomyopathy
• Chest pain lasting less than 10 minutes
8. Chronic Stable angina
is due to inability to supply the myocardium
(heart muscle) with sufficient blood in situation
of increased cardiac output (such as
exertion).due to
1-Atherosclerosis
2- coronary vasospasm may occur at the site of a
lesion
3-less frequently normal vessels
4-congenital ,emboli, arthritis ,dissection of
aorta or infarction,
9. Angina may also occur by
-Hypertrophy cardiomyopathy
-Aortic stenosis,
-Aortic regurgitation,
-Hyperthyroidism ,
-Anemia ,
-PAT, V.tach,
Another kind of Angina called X –syndrom
Which cause by (microvasculature disease ) is
difficult to diagnosis.
Treatment is often not succeful,
prognosis is good
12. Prinzmetal (variant)Angina
• Is a syndrome – usually results from coronary
vasoconstriction
• It tends to involve mostly RCA ,and there may
be no fixed stenosis
• Chest pain may occur with out precipitating
factor
• Is associted St.segment elelvation rather than
deprssion
• Mostly affect womens under 50years of age
13. • Mostly occur early morning ,awake patient
from sleep ,may be with arrhythmias
Treatment
• Aggressive medical treatment
,revascularization, if no stenosis than stop
smoking or
• use of cocaien precipitate pain
• Respond well with nitrate-Ca chanel blockers
( ,nifidipien,diltiazem,amlodipine)
• Beta blocker,
14. Canadian CV society functional
classification of stable angina
Grade 1-
physical activity, walking,climbing staires,not
cause angina
Grade2-
Slight limitation of ordinary activity
Walking or climbing stairs rapidly ,walking up
hill,in cold ,in wind,or when in under
emotional stress ,or after heavy meals or after
walking few hours after walking cause pain
15. Grade 3
Marked limitation of ordinary physical activity
walking 1-3 blocks on the level
And climbing less than one flight in normal
condition
Grade 4-
• Inability to carry on any physical activity with
out discomfort ,angina ,may be present at rest
16. Symptoms
Depend of
• past history
• Circumstances (activities, relief by rest)
Character of pain
Pt .not refer angina as pain,
but as sensation,tightness,squeezing,burning
,pressing,choking,aching,bursting,gas
(indigestion),
Some times clenching in the middle of chest.
Location and radiation
.duration is short less than 3minute
19. Is in short duration ,
Some times start after heavy meals
If more than 30 minutes than MI,
unstable angina reliev by taking Nitro-And
diagnositic .relieve and subsides
SIGNS.
Bp may up or down,
tachycardia or more bradycardia
Gallop rhythm,
sysytolic murmur(MR,papilary muscle dysfunction)-
-SVT,or V.Tach
20. Diagnosis
• Lab-(CK-MB),Troponin ,Anemia
,Hyperlipdemia
• ECG- some time normal,or st depresion ,T
wave inversion or flatened T waves,
• History ,clinical symptomes,
• Non invassive TMT is important bruce
protocole
• Or TMT- stress echo-nuclear ,MRI
21. Stress test
Precaution –indication –contra indication
• Myocardial stress imaging
-when TMT not gave us final result-LBBB
-when clinical and test is not matching
-to localize the region
-to assess the completeness of vascularization
after bypass or angiogram
-as prognostic indicator with any known CAD
22. .ACS (Acute coronary syndrom)
Unstable angina,
STEMI and NSTEMI are attributed to
"plaque rupture", where one of the
plaques gets weakened, develops a tear,
and forms an adherent blood clot that
either obstructs blood flow or floats
further down the blood vessel, causing
obstruction there
23. Effect Of Ischemia
• (IHD) Ischeamic heart disease may be present
with any of the following problems:
• Angina pectoris
(chest pain on exertion, in cold weather or
emotional situations)
• Acute chest pain:
(ACS)acute coronary syndrome, unstable angina or
myocardial infarction("heart attack", severe chest
pain unrelieved by rest associated with evidence
of acute heart damage)
• Heart failure
• (difficulty in breathing or swelling of the
extremities due to weakness of the heart muscle)
24. Diagnosis
• The diagnosis of ischaemic heart disease
underlying particular symptoms depends largely
on the nature of the symptoms.
• The first investigation is an electrocardiogram
(ECG/EKG), both for "stable" angina and acute
coronary syndrome.
• An X-ray of the chest
• Blood tests may be performed.
• Myeloperoxidase has been proposed as a
biomarker
25. Prevention
• Various treatments are offered in people
deemed to be at high risk of coronary artery
disease.
• These include control of cholesterol levels in
those with known high cholesterol,
• smoking cessation,
• dietary intervention (especially eating more
vegetables and less meat),[
• and control of high blood pressure.
• Regular Exercise
26. Management
• In stable IHD,
• Anti anginal drugs may be used to reduce the rate
of occurrence and severity of angina attacks.
• Treatments for acute coronary syndrome and
established coronary artery disease is discussed
above in "diagnosis".
• Revascularization for acute coronary syndrome
has a significant mortality benefit.
• Recent evidence suggests that revascularization
for stable ischeamic heart disease may also
confer a mortality benefit over medical therapy
alone.[]
27. • Treatment of coronary artery disease includes
addressing "modifiable" risk factors.
• This includes suppression of cholesterol
(usually with statins), even in those with
statistically normal cholesterol levels, control
of blood pressure, blood sugars (if diabetic),
and regular exercise.
• Smokers are encouraged to stop smoking.
• Diet plays a major role in the progression of
coronary artery disease and by making certain
diet choices a person can drastically change
their chance of dying from it.
28. Treatment
• Drug therapy is commonly used for treatment of
ischemic heart disease and includes:
• Angiotensin receptor blockers (ARBs), which lower
blood pressure,losartan
• Anti-ischemic agents such as ranolazine (Ranexa)
• Antiplatelet drugs, which prevent the formation of
blood clots
• Beta-blockers, which lower the heart rate
• Calcium channel blockers, which reduce workload on
the heart muscle
• Nitrates, which dilate the blood vessels
• Statins, which lower cholesterol
29. • Surgical procedures used to treat ischemic
heart disease
• Severe symptoms that are not relieved by
medication alone are treated with surgical
procedures including:
• Angioplasty and stent placement (procedure to
remove plaque and restore blood flow in
clogged arteries)
• Coronary artery bypass graft (procedure that
helps restore blood flow to the heart by routing
the flow through transplanted arteries)
30. • What you can do to improve your ischemic
heart disease
• In addition to following your treatment
plan, you may be able to improve your
ischemic heart disease by:
• Getting regular physical activity
• Keeping your cholesterol at a healthy level
• Maintaining normal blood pressure
• Quitting tobacco use
• Reducing cholesterol and fat in your diet
31. • What are the potential complications of
ischemic heart disease?
• You can help minimize your risk of serious
complications by following the treatment plan
you and your health care professional design
specifically for you.
Complications of ischemic heart disease
include:
• Arrythmia (irregular heart rhythm)
• Heart damage
• Myocardial infarction (heart attack)