Uterine inversion occurs when the uterus turns inside out, most commonly during the third stage of labor due to excessive traction on the umbilical cord or fundal pressure. It can be incomplete, with just the fundus inverted, or complete, with the entire uterus emerging from the vagina or outside the body. Symptoms include hemorrhage, abdominal pain, and shock. Treatment involves immediate manual repositioning of the uterus if diagnosed early, or the O'Sullivan hydrostatic method using saline if delayed. Prevention relies on avoiding excessive fundal pressure or cord traction during delivery of the placenta.
When fetal head is delivered, but shoulders are stuck and cannot be delivered it is known as shoulder dystocia.
The anterior shoulder becomes trapped behind on the symphysis pubis, whilst the posterior shoulder may be in the hollow of the sacrum or high above the sacral promontory.
This ppt is made by Mr. arkab khan pathan under guidance of Mrs. RAKHI GOAR. this ppt contain the detail and all the lecture notes of HEG.
THANK YOU.
Arkab khan
Please find the power point on Management of Preterm labor. I tried to present it on understandable way and all the contents are reviewed by experts and from very reliable references. Thank you
This topic contains definition, incidence, varieties, causes, risk factors, dangers, diagnosis, prognosis, prevention and management of inversion of uterus.
Retained placenta can be defined as lack of placental expulsion within 30 minutes of delivery of an infant. it is more common in preterm. Retained Placenta can lead to massive PPH and increase maternal morbidity and mortality.
When fetal head is delivered, but shoulders are stuck and cannot be delivered it is known as shoulder dystocia.
The anterior shoulder becomes trapped behind on the symphysis pubis, whilst the posterior shoulder may be in the hollow of the sacrum or high above the sacral promontory.
This ppt is made by Mr. arkab khan pathan under guidance of Mrs. RAKHI GOAR. this ppt contain the detail and all the lecture notes of HEG.
THANK YOU.
Arkab khan
Please find the power point on Management of Preterm labor. I tried to present it on understandable way and all the contents are reviewed by experts and from very reliable references. Thank you
This topic contains definition, incidence, varieties, causes, risk factors, dangers, diagnosis, prognosis, prevention and management of inversion of uterus.
Retained placenta can be defined as lack of placental expulsion within 30 minutes of delivery of an infant. it is more common in preterm. Retained Placenta can lead to massive PPH and increase maternal morbidity and mortality.
“Difficulty encountered in the delivery of the fetal shoulders after delivery of the head.”
Shoulder dystocia is an unpredictable obstetric complication with the incidence of 0.15% to 2%.
An increase in the incidence of shoulder dystocia has been recorded over the last 20 years. Incidence appears to be increasing as birth weights increase.
It is the expulsion or extraction from its mother of an embryo or fetus weighing 500 gm or less when it is not capable of independent survival (WHO).
The 500gm of fetal development is attained approximately at 22 weeks of gestation.
Expelled fetus- Abortus
Emergencies that occur in pregnancy or during or after labor and delivery.
main emergencies are
Ectopic Pregnancy
Uterine Inversion
Obstetrical Shock
Cord Prolepses
Amniotic Fluid Embolism
Postpartum Hemorrhage
Obstetrics and Gynecological Nursing
The PPT contains detailed information about Abnormal uterine action, its classifications, causes, sign and symptoms and management.
Abnormal uterine action is the one of the factors causing dystocia in which uterine forces are insuffiently strong or inappropriate coordinated to efface and dilate the cervix. Pelvic contraction is often accompanied by uterine dysfunction and the two together constitute the most common cause of dystocia.
Uterus Is thick muscular walls adapt to the growth of the fetus and then pro...tekalignpawulose09
The non-gravid (not pregnant) uterus is approximately 7.5 cm
long, 5 cm wide & usually lies in the lesser pelvis (during
pregnancy, it is abdominal organ)
but the size, thickness & position varies considerably during
the various changes of life
Nsg care with Fluid & Electrolyte imbalance.pptxAbhishek Joshi
Helpful for first year GNM and B.Sc. Nurses students.
Keep Reading and i will keep uploading...i want to enhance the nursing profession and provide an ideal nursing care to one and every students of India. Thanks
i have prepared this ppt. from various Books as a refrences as well as uses of web pages and explain and modify in simplify language which are easily understand by medical or para medical personnel..thank you..
this power point presentation is made ideally according to criteria of ppt. with opener , energizes , bibliography ans much more criteria are followed.thank you..
it is a short and essential details regarding levels of prevention in Community health Nursing.and this ppt is most important for Nurses especially for post basic B.S.Sc.nursing students , because all criteria of power point presentation are followed in this ppt file.please like , share and improve your knowledge.thank you...
How to Make a Field invisible in Odoo 17Celine George
It is possible to hide or invisible some fields in odoo. Commonly using “invisible” attribute in the field definition to invisible the fields. This slide will show how to make a field invisible in odoo 17.
Students, digital devices and success - Andreas Schleicher - 27 May 2024..pptxEduSkills OECD
Andreas Schleicher presents at the OECD webinar ‘Digital devices in schools: detrimental distraction or secret to success?’ on 27 May 2024. The presentation was based on findings from PISA 2022 results and the webinar helped launch the PISA in Focus ‘Managing screen time: How to protect and equip students against distraction’ https://www.oecd-ilibrary.org/education/managing-screen-time_7c225af4-en and the OECD Education Policy Perspective ‘Students, digital devices and success’ can be found here - https://oe.cd/il/5yV
The Roman Empire A Historical Colossus.pdfkaushalkr1407
The Roman Empire, a vast and enduring power, stands as one of history's most remarkable civilizations, leaving an indelible imprint on the world. It emerged from the Roman Republic, transitioning into an imperial powerhouse under the leadership of Augustus Caesar in 27 BCE. This transformation marked the beginning of an era defined by unprecedented territorial expansion, architectural marvels, and profound cultural influence.
The empire's roots lie in the city of Rome, founded, according to legend, by Romulus in 753 BCE. Over centuries, Rome evolved from a small settlement to a formidable republic, characterized by a complex political system with elected officials and checks on power. However, internal strife, class conflicts, and military ambitions paved the way for the end of the Republic. Julius Caesar’s dictatorship and subsequent assassination in 44 BCE created a power vacuum, leading to a civil war. Octavian, later Augustus, emerged victorious, heralding the Roman Empire’s birth.
Under Augustus, the empire experienced the Pax Romana, a 200-year period of relative peace and stability. Augustus reformed the military, established efficient administrative systems, and initiated grand construction projects. The empire's borders expanded, encompassing territories from Britain to Egypt and from Spain to the Euphrates. Roman legions, renowned for their discipline and engineering prowess, secured and maintained these vast territories, building roads, fortifications, and cities that facilitated control and integration.
The Roman Empire’s society was hierarchical, with a rigid class system. At the top were the patricians, wealthy elites who held significant political power. Below them were the plebeians, free citizens with limited political influence, and the vast numbers of slaves who formed the backbone of the economy. The family unit was central, governed by the paterfamilias, the male head who held absolute authority.
Culturally, the Romans were eclectic, absorbing and adapting elements from the civilizations they encountered, particularly the Greeks. Roman art, literature, and philosophy reflected this synthesis, creating a rich cultural tapestry. Latin, the Roman language, became the lingua franca of the Western world, influencing numerous modern languages.
Roman architecture and engineering achievements were monumental. They perfected the arch, vault, and dome, constructing enduring structures like the Colosseum, Pantheon, and aqueducts. These engineering marvels not only showcased Roman ingenuity but also served practical purposes, from public entertainment to water supply.
Instructions for Submissions thorugh G- Classroom.pptxJheel Barad
This presentation provides a briefing on how to upload submissions and documents in Google Classroom. It was prepared as part of an orientation for new Sainik School in-service teacher trainees. As a training officer, my goal is to ensure that you are comfortable and proficient with this essential tool for managing assignments and fostering student engagement.
Read| The latest issue of The Challenger is here! We are thrilled to announce that our school paper has qualified for the NATIONAL SCHOOLS PRESS CONFERENCE (NSPC) 2024. Thank you for your unwavering support and trust. Dive into the stories that made us stand out!
The Indian economy is classified into different sectors to simplify the analysis and understanding of economic activities. For Class 10, it's essential to grasp the sectors of the Indian economy, understand their characteristics, and recognize their importance. This guide will provide detailed notes on the Sectors of the Indian Economy Class 10, using specific long-tail keywords to enhance comprehension.
For more information, visit-www.vavaclasses.com
How to Create Map Views in the Odoo 17 ERPCeline George
The map views are useful for providing a geographical representation of data. They allow users to visualize and analyze the data in a more intuitive manner.
2. OBJECTIVES
1. To learn about uterine inversion
2. To learn how to diagnose uterine inversion
3. To Learn what are are the causes of
uterine inversion
4. To learn What are the Treatment of Uterine
Inversion
5. Steps to manage uterine inversion
3. Content
Introduction Of Topic
Definition
Classification of Inversion of Uterus
Degrees
Causes
Pathophysiology
Sign & Symptoms
Diagnosis
Management
Prevention
4. Introduction
This is Rare.But Potentially Life
Threatening Complication of the Third
Stage Of Lobour.
It Occurs in Approximately 1 in 20,000
Deliveries
The Obstetric Inversion is almost always
an Acute One & Usually Complete.
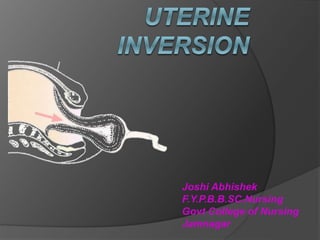
5. DEFINITION
‘‘ When Uterus Turns Inside Out, It Is
Called Uterine Inversion.”
‘‘Inversion of Uterus means Uterus is
Turned Inside Out Partially OR
Completely.
Uterine inversion is the folding of the
fundus into the uterine cavity in varying
degrees.
6. CLASSIFICATION
Inversion Of Uterus is Classified in
Mainly 3 Types :
A. According Types
B. According Degrees
C. According the Timing of Event
7. A. Types
1) Incomplete Inversion :
When fundus of uterus has turned
inside out, like toe of socks, but inverted
fundus has not descended through Cx…
2) Complete Inversion :
When the inverted fundus has
passed completely through Cx to lie
within the vagina or lie often outside the
Vaginal Wall.
8.
9. B. Degrees
First degree: The uterus is partially
turned out
Second degree: The fundus has passed
through the cervix but not outside the
vagina
Third degree: The fundus is prolapsed
outside the vagina
Fourth degree: The uterus, cervix and
vagina are completely turned inside out
and are visible
10. Universally….
First Degree : Incomplete Inversion
Second Degree : Complete inversion in
the vagina
Third Degree : Complete inversion
outside the Vagina
11. 1st Degree
- Inverted fundus
up to cervix
2nd Degree
- Body of uterus
protrudes through
cervix into vagina
3rd Degree
- Prolapse of
inverted uterus
outside vulva
12.
13. C. According to Timing of
Event
Acute : It occurs within 24 hrs of
delivery.
Sub-acute : It presents between 24 hrs
& 4 wks of delivery.
Chronic : It presents beyond 4 wks of
delivery or in non pregnant stage.
14. CAUSES
Excessive cord traction (esp. with an
unseparated placenta)
Excessive fundal pressure (esp. when
uterus is poorly contracted Atonic)
Placenta accreta
Congenital predisposition
Fundal implantation of placenta
Either Spontaneous OR Iatrogenic
causes.
15. Conti…
Spontaneous (40%) :
Abnormal short umbilical cord or
functionally shortened by being wrapped
around the fetal body.
Sudden rise in intra abdominal pressure
due to maternal coughing or vomiting.
Morbid adherence of fundally implanted
placenta
Connective tissue disorder such as
Marphan’s syndrome.
16. Conti…
Latrogenic:
Due to mismanagement of third stage of labor…
Pulling the cord when the uterus is atonic while
combined with fundal pressure
Crede’s Expression while the uterus is relaxed
Faulty technique in manual removal of placenta
While separating retained placenta from the wall, a
portion may remain attached and as the placenta
is withdrawn, the fundus is also withdrawn.
17. PATHOPHYSIOLOGY
a portion of uterine wall prolapses through the
dilated cervix or indents forward
relaxation of part of the uterine wall
simultaneous downward traction on the fundus
leading to inversion of the uterus.
18. Sign & Symptoms
Hemorrhage (94%)
Severe abdominal pain in 3rd stage
Hypotension with Bradycardia: shock out of
proportion to the blood loss (neurogenic due to
increased vagal tone)
Uterine fundus not palpable abdominally
Mass in the vagina on vaginal examination.
Sudden cardiovascular collapse
Lump in the vagina
Abdominal tenderness
Absence of uterine fundus on abdominal palpation
19. Conti…
Shock
Shock is initially out of proportion with the amount
of blood loss.
Woman becomes sweaty with bradycardia,
profound hypotension and rarely cardiac arrest.
In short time there is marked hemorrhage and
Hypovolemic shock.
20. DIAGNOSIS
The diagnosis of uterine inversion is based
upon clinical findings:
Bleeding, which may be severe and result in
Hemorrhagic Shock
Palpation of the prolapsed uterine fundus:
Lower uterine segment = INCOMPLETE
Vagina = COMPLETE
By Intra Uterine Manual Examination
21. DIFFRENTIAL DIAGNOSIS
Inversion of uterus
Uterine rupture.
Prolapse of uterine tumor (submucous
fibroid).
Large endometrial polyp.
Passage of succenturiate lobe of placenta.
23. Uterine Inversion
Remove placenta
Oxytocic infusion
(40 units/500mls
NS)
Antibiotics observe
O’Sullivan hydrostatic method
-dependent part replace into
vagina
-5L or more physiological
solution deposited onto
posterior fornix
-assistant create water tight
seal
Manual reduction
-apply pressure to
dependent part of
uterus
-simultaneous
pressing with other
hand on other part
which inverted last
GA/ stabilize
patient
UTERUS
REPLACED
Immediate
replacement
Resuscitate, IV
access, fluids/ bolus
replacement
NOYES
24. Conti…
Teamwork = resuscitation + uterine
repositioning simultaneously
postpartum hemorrhage drill.
The quickest way to treat neurogenic
shock - to replace the uterus.
25.
26.
27. Mx of Acute Inversion of Uterus
Delay in treatment increases the mortality, So
number of steps are taken immediately and
simultaneously.
Before shock develops :
When one is on the spot when the inversion happens
TRY IMMEDIATE MANUAL REPLACEMENT, even
without anesthesia if not easily available.
Principle :
“ The part of the uterus which has come
down last , should go back first. “
28. Procedure
If the diagnosis is made immediately after
the inversion has occurred, then that same
degree of relaxation of myometrium and
cervix (which is required for the inversion to
occur) will allow uterine replacement
easily…
1. The gloved hand is lubricated with suitable
antiseptic cream and placed inside the vagina.
2. The uterine fundus with or without the
attached placenta, is cupped in the palm of the
hand. The fingers and thumb of the hand are
extended to identify margins of the cervix.
29. 3. The whole uterus is
lifted upwards towards
and beyond umbilicus
4. Additional pressure is
exerted with the
fingertips systematically
and sequentially to
push and squeeze the
uterine wall back
through the cervix.
29Dr Shashwat Jani. 9909944160
30. 5. Sustained pressure for 3-5 mins to achieve
complete replacement
6. Apply counter support by the other hand
placed on the abdomen
7. Once the fundus has been replaced keep
the hand in the uterus while rapid infusion
of oxytocin is given to contract the uterus.
Initially, bimanual compression aids in
control of further hemorrhage until uterine
tone is recovered.
31. 8. When the uterus is felt contracting, the hand
is slowly withdrawn.
If placenta is attached, it is to be removed only
after the uterus becomes contracted.
If the placenta is partially attached , it should
be peeled out before replacement of uterus.
32.
33. 1) Starting from the edge of placenta ,
2) The placenta is separated by
a) keeping the back of the hand in contact with the
uterine wall.
b) with slicing movement of the hand.
33Dr Shashwat Jani. 9909944160
34. O’Sullivan’s hydrostatic
method
Tube passed into the
posterior fornix
Assistant close vulva
around operator’s wrist
Warm saline run in
until pressure gradually
restores position of
uterus
37. Alternatively the tubing can be attached to
sialistic vacuum extracter cup which is placed
inside introitus and may provide better seal.
As the vaginal wall distends, there is increase
in intravaginal pressure, the fundus of uterus
rises and inversion is corrected
Once this is achieved, fluid is allowed to escape
slowly from vagina.
Dr Shashwat Jani. 9909944160 37
38.
39. Conti…
If this technique fails, Haultain's Operation
can done.
In this following steps are taken:
Exteriorize the uterus
Cervical ring may be stretched
42. SPINELLI’S METHOD
Anterior Colostomy is done and incision
on the constricting cervical ring is given
for the replacement of uterus .
43. KUSTNER’S METHOD
Posterior Colpotomy is done and incision of the
cervix similar to that of spinelli’s method.
43
44. Hysterectomy
Failure of conservative surgery
Family is completed
sepsis
Dr Shashwat Jani. 9909944160 44
45. MANEUVERS : TO BE AVOIDED
Excessive traction on the umbilical cord
Excessive fundal pressure
Excessive intra-abdominal pressure
Excessively vigorous manual removal of
placenta.
45Dr Shashwat Jani. 9909944160
46.
47. Prevention
Do not employ any method to expel the
placenta when the uterus is relaxed
Patient should not be instructed to change her
position.
Pulling the cord simultaneously with fundal
pressure should be avoided
Manual removal of placenta should be done in
proper manner.
47Dr Shashwat Jani. 9909944160
48. Bibliography
1. D.C. DATTA’S ; ‘‘A TEXT BOOK OF OBSTETRICS’’
SEVENTH EDITION;PUBLISHED BY NEW CENTRAL BOOK AGENCY
MEDICAL PUBLISHERS (P) LIMITED;KOLKATA;
P.NO.420 TO 421.
2.PV BOOKS; ‘‘ A TEXT BOOK OF MATERNAL HEALTH NURSING’’
FIFTH EDITION;EDITED BY R.K.GUPTA;P.NO. TO 500.
3.MYLES; ‘‘A TEXT BOOK FOR MIDWIVES’’ SIXTEENTH EDITION;
INTERNATIONAL EDITION;PUBLISHED BY SAUNDERS ELSEVIER;
EDITED BY JAYNE MARSHALL & MAUREEN RAYNOR
P NO.- 510 TO 515
4. WEBPAGE; ‘‘WWW.WIKIPEDIA.COM & WWW.ENCYCLOPEDIA.COM’’;
TOPIC OF UTERINE INVERSION ;TEXT AND PICTURES OF ANAEMIA
BY DR.KIRAN SADHU,R.N.R.M PROFESSOR.
5. WEBPAGE;‘‘WWW.GOOGLE.COM & WWW.SLIDESHARE.COM”;
TOPIC OF UTERINE INVERSION;TEXT AND PICTURES;BY
RUCHITA BHATT,R.N.R.M.LECTURER