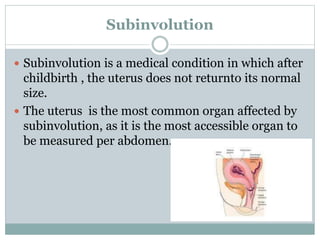
The document discusses minor discomforts and complications that can occur during the postpartum period known as the pueperium. It defines pueperium as the 6-week period following childbirth where the body reverts to its pre-pregnant state. Common minor discomforts include afterpains, perineal pain, breast engorgement, increased urination, and constipation. Potential complications include postpartum hemorrhage, puerperal pyrexia (fever), puerperal sepsis (infection), urinary tract infections, and subinvolution where the uterus does not return to normal size. The document provides information on causes, signs, symptoms, and management of these minor discomforts




















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















