Downloaded 194 times
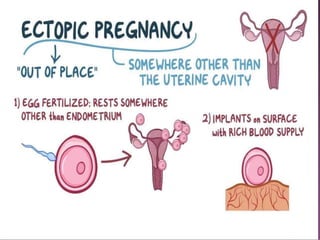
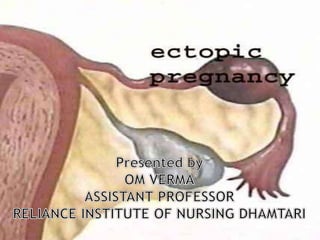
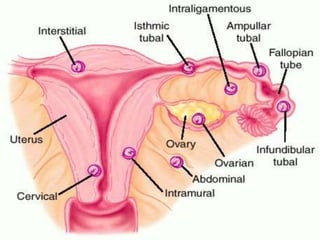
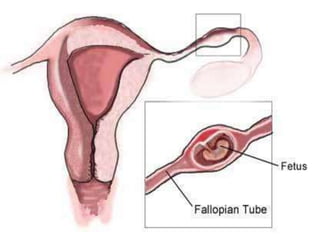



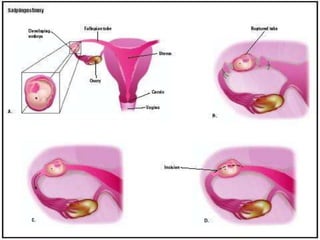



An ectopic pregnancy occurs when a fertilized egg implants and grows outside the uterus, usually in one of the fallopian tubes. This is a medical emergency that requires prompt treatment to stop potentially life-threatening bleeding. Most ectopic pregnancies occur in the fallopian tubes. While the incidence of ectopic pregnancy is rising due to increased rates of pelvic inflammatory disease, early diagnosis and treatment have reduced maternal death and illness.























































































