Downloaded 775 times




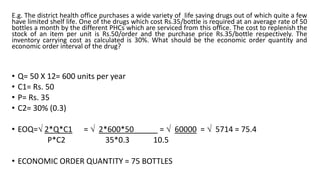

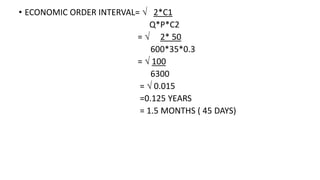
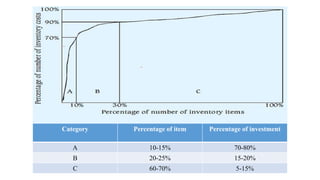
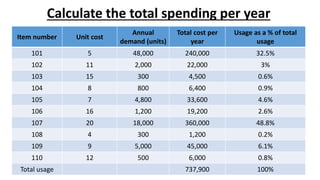
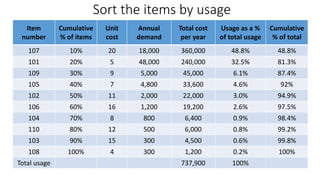
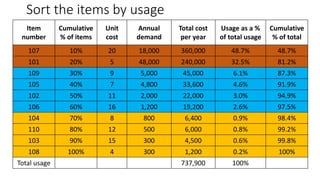
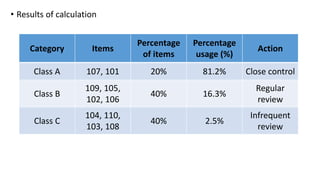
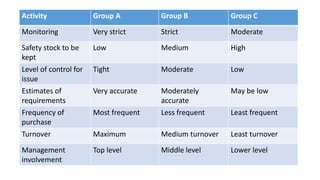

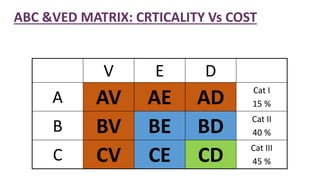



The document discusses inventory management principles including definitions, objectives, costs, and models. It summarizes key concepts like ABC analysis which categorizes inventory items into A, B, and C groups based on their value and usage. Group A items account for 20% of items but 80% of cost, requiring close control, while Group C items are less important with loose control. The document also covers economic order quantity and interval models to determine optimal reorder amounts and times.



















































































![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)














