Downloaded 1,004 times
























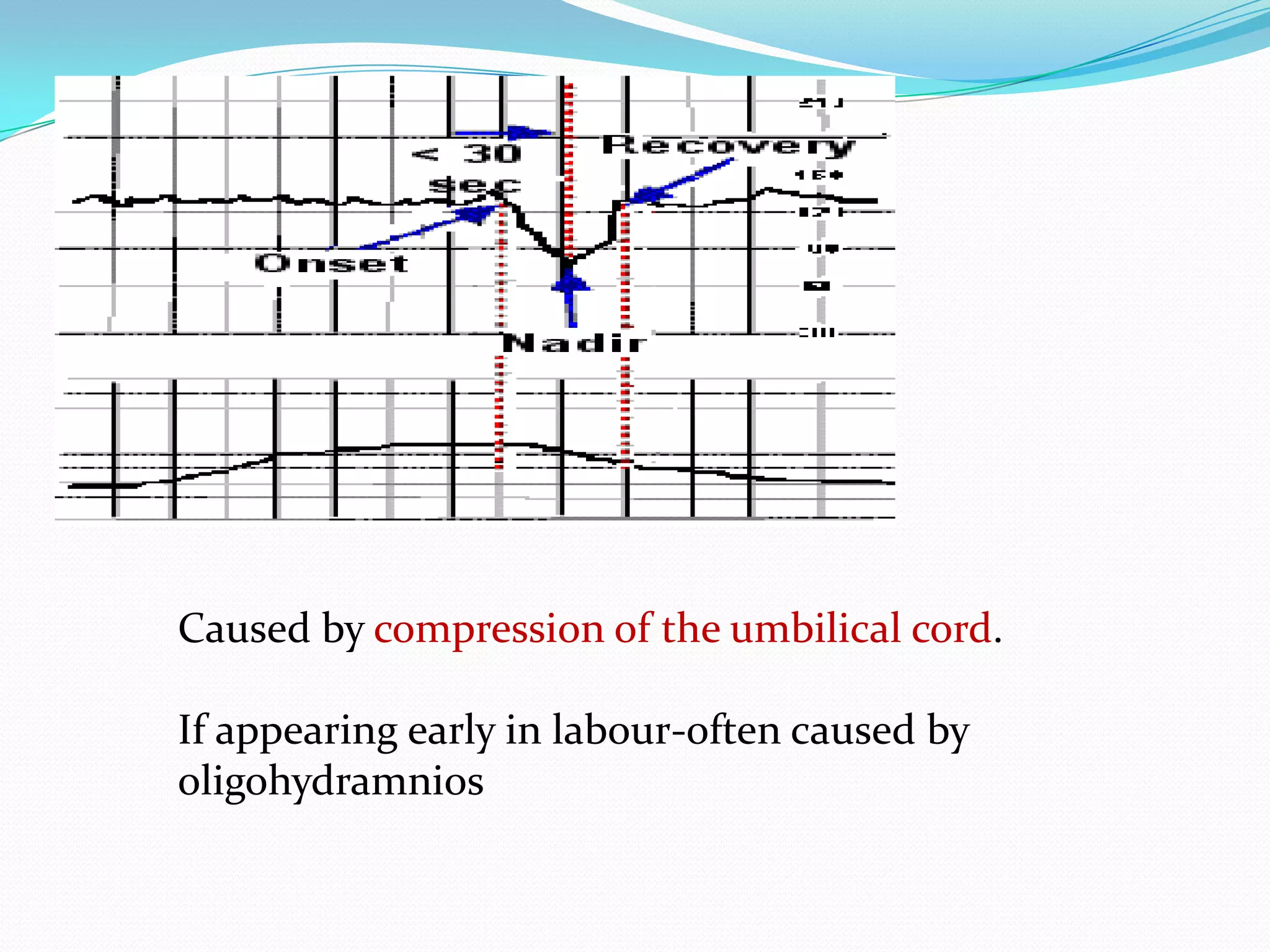





















This document provides information on intrapartum fetal monitoring techniques including fetal heart rate monitoring, indications for continuous electronic fetal monitoring, interpretation of fetal heart rate patterns, and management of non-reassuring fetal status. It discusses techniques like intermittent auscultation, electronic fetal monitoring, fetal scalp pH testing, pulse oximetry, and lactate testing. The goal of intrapartum monitoring is timely identification and rescue of fetuses at risk for neonatal morbidity from hypoxic insult during labor and delivery.












































































