Download as PDF, PPTX













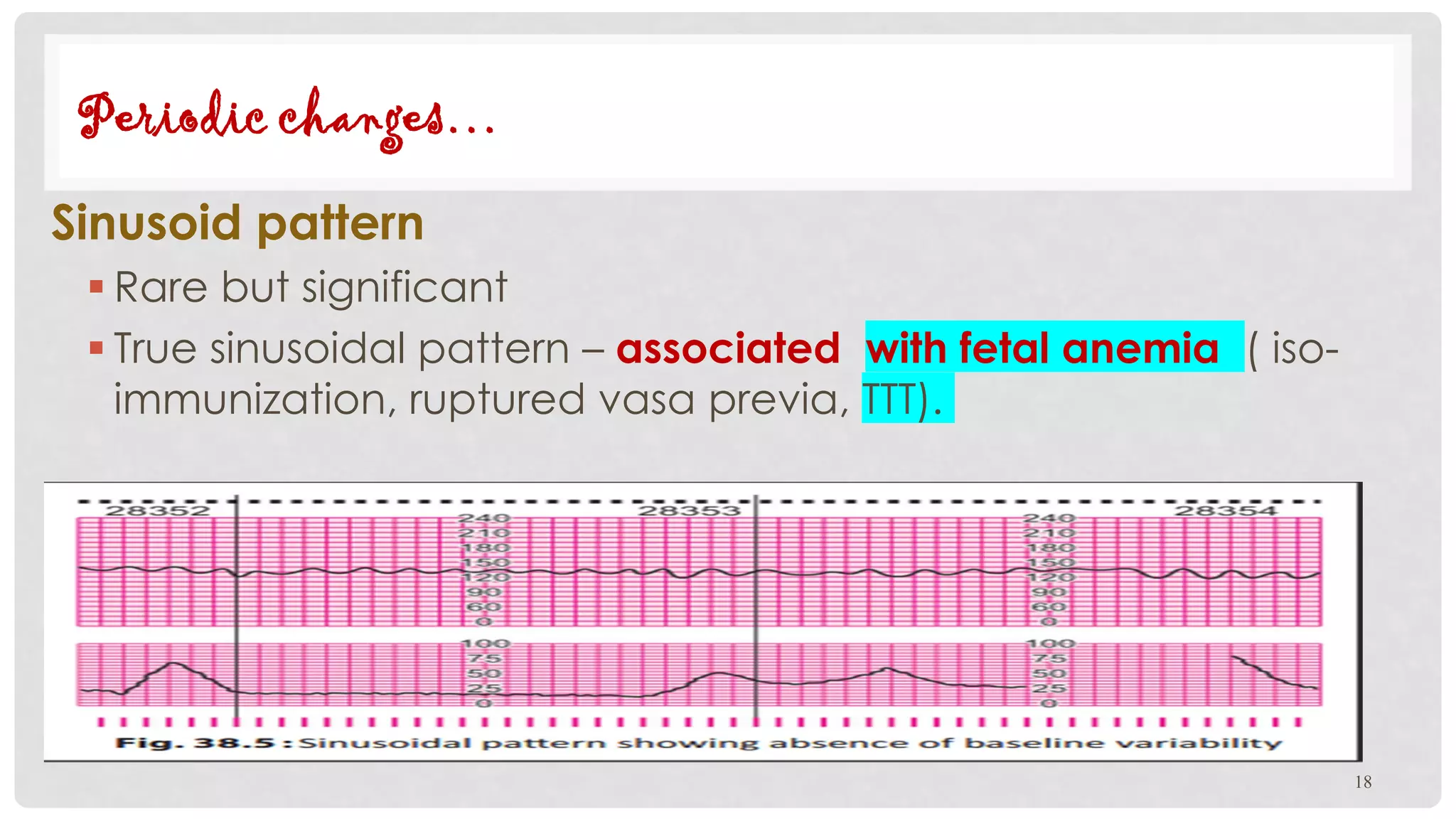




This document discusses fetal heart rate monitoring techniques and patterns. It describes intermittent auscultation using a fetoscope or Doppler ultrasound, and continuous electronic fetal monitoring using cardiotocography. Normal fetal heart rate is between 120-160 bpm; patterns like late decelerations, variable decelerations, or a sinusoidal pattern are non-reassuring. The document outlines how to interpret and manage different fetal heart rate patterns.
















































![Abnormal Labor [ Natnael Dechasa Gemeda pdf ].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/abnormallabornatnaeldechasagemedapdf-230317103358-a4021124-thumbnail.jpg?width=640&height=640&fit=bounds)






![Obstetric Anesthesia ppt [ Natnael Dechasa ].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/obstetricanesthesiapptnatnaeldechasa-230310124013-7b6867cb-thumbnail.jpg?width=640&height=640&fit=bounds)





![Natnael Dechasa Gemeda [Pictures ].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/natnaeldechasagemedapictures-230407125448-70db55fc-thumbnail.jpg?width=640&height=640&fit=bounds)






















