The document provides definitions and descriptions of key terms used in cardiotocography (CTG) including:
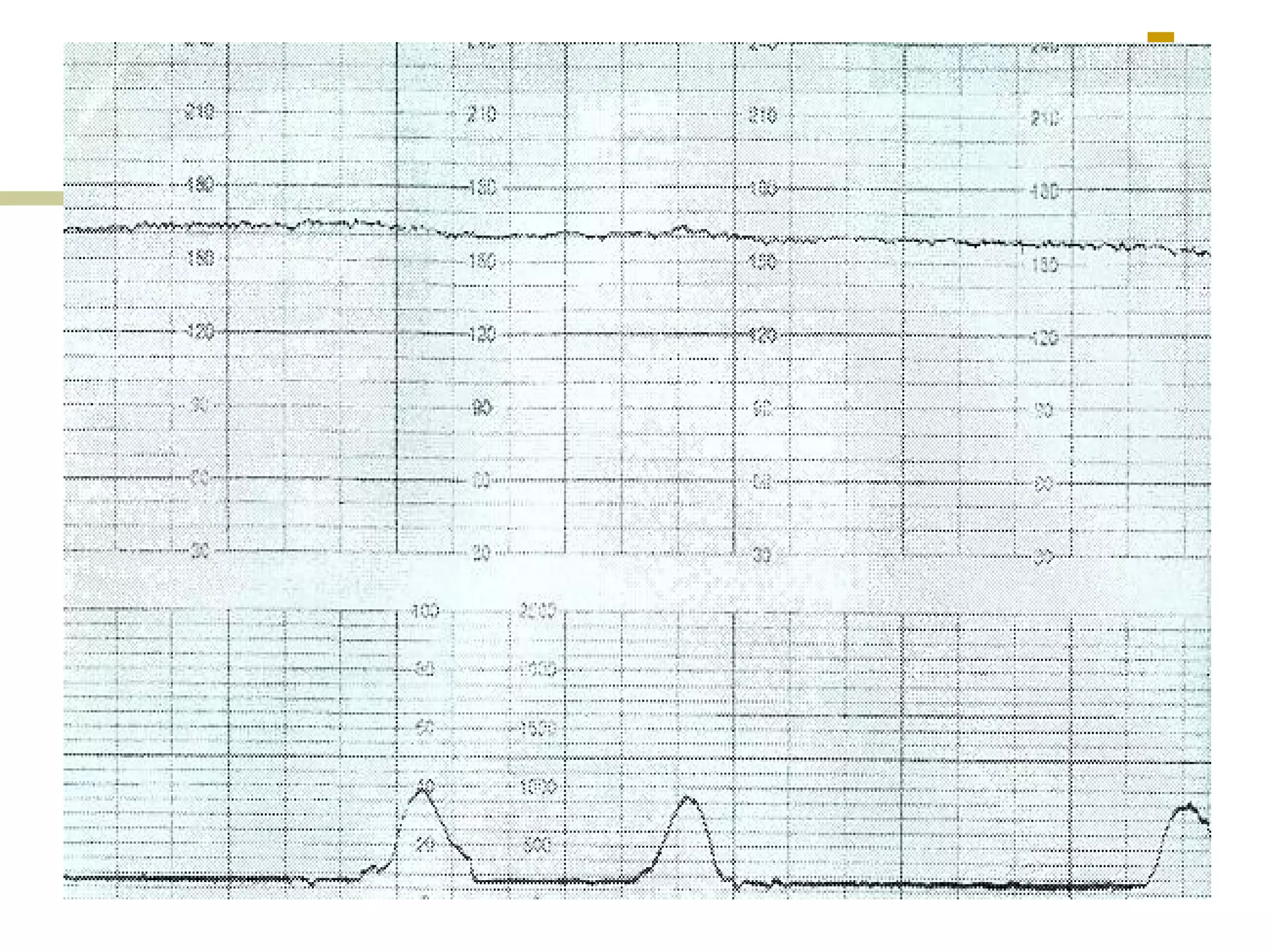
- Baseline heart rate, acceleration, deceleration, variability
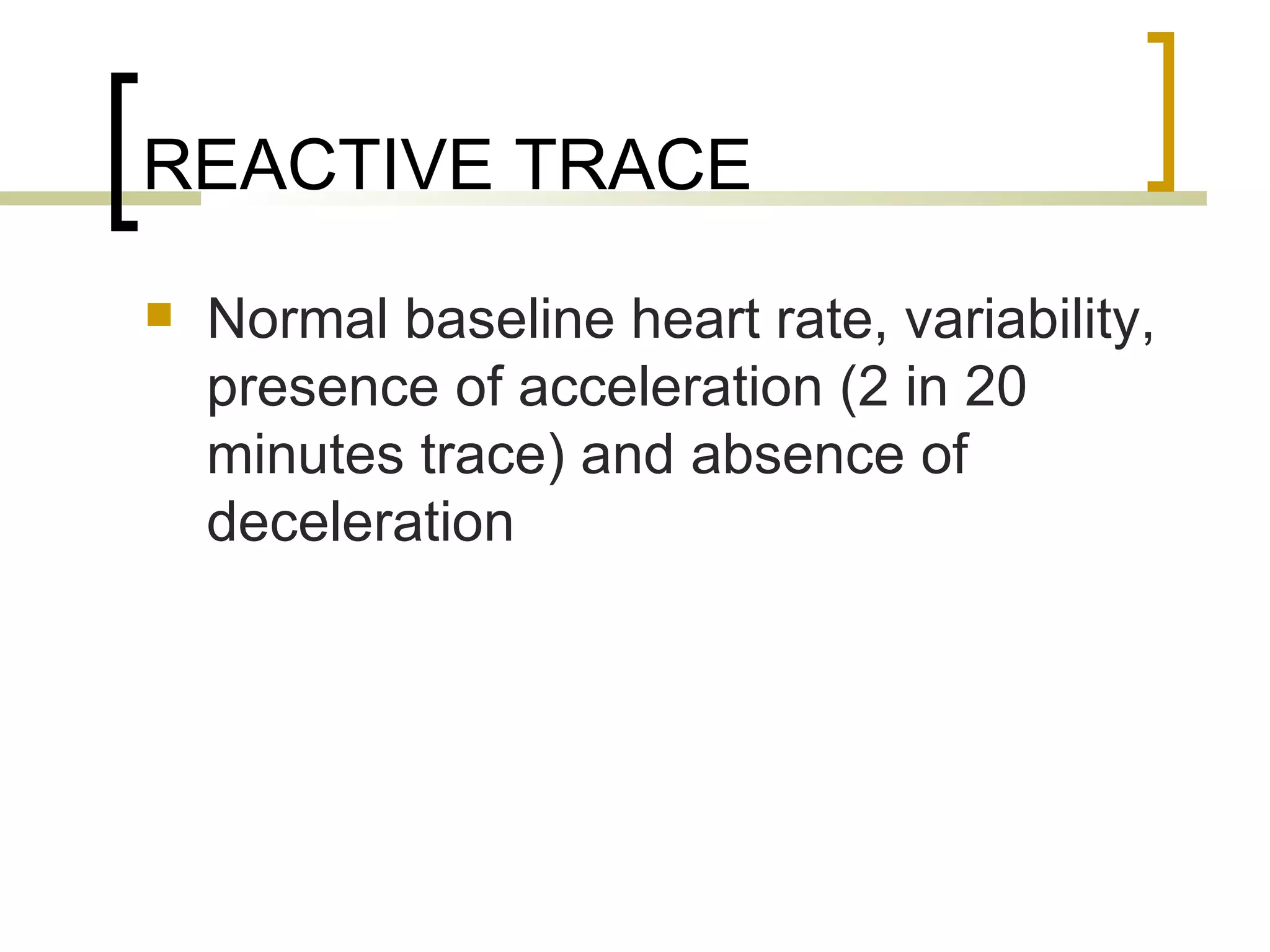
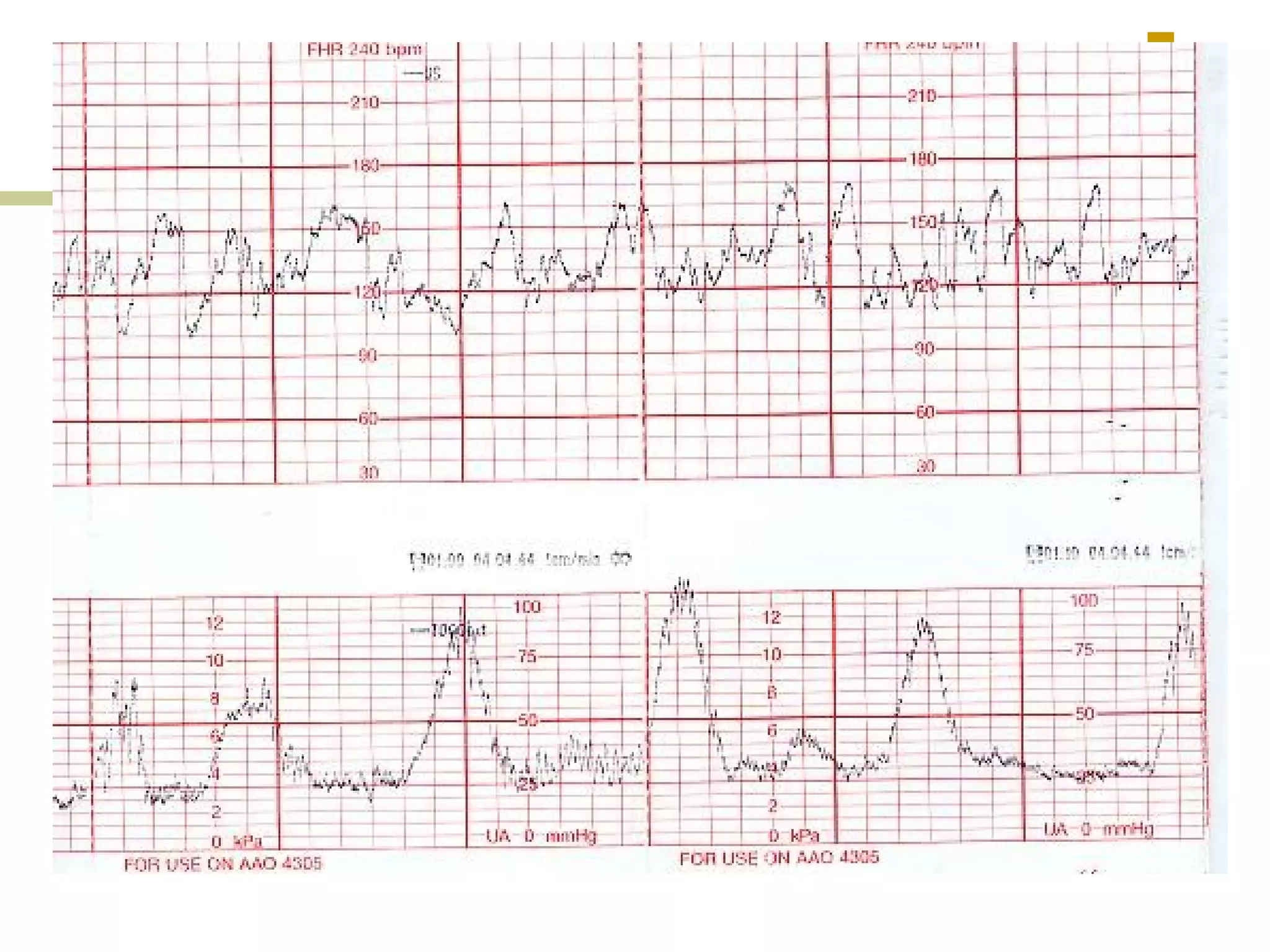
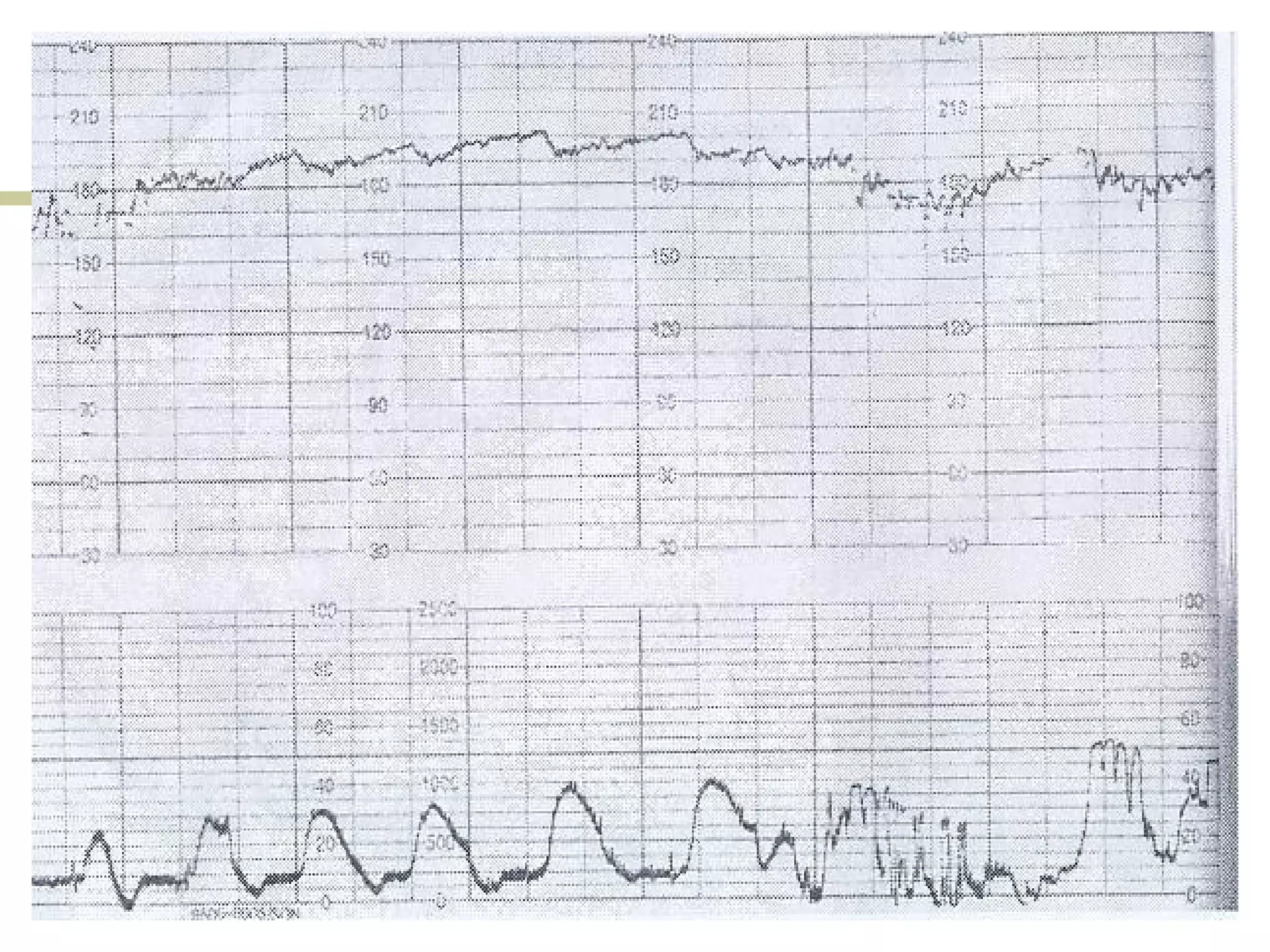
- Reactive, bradycardia, tachycardia traces
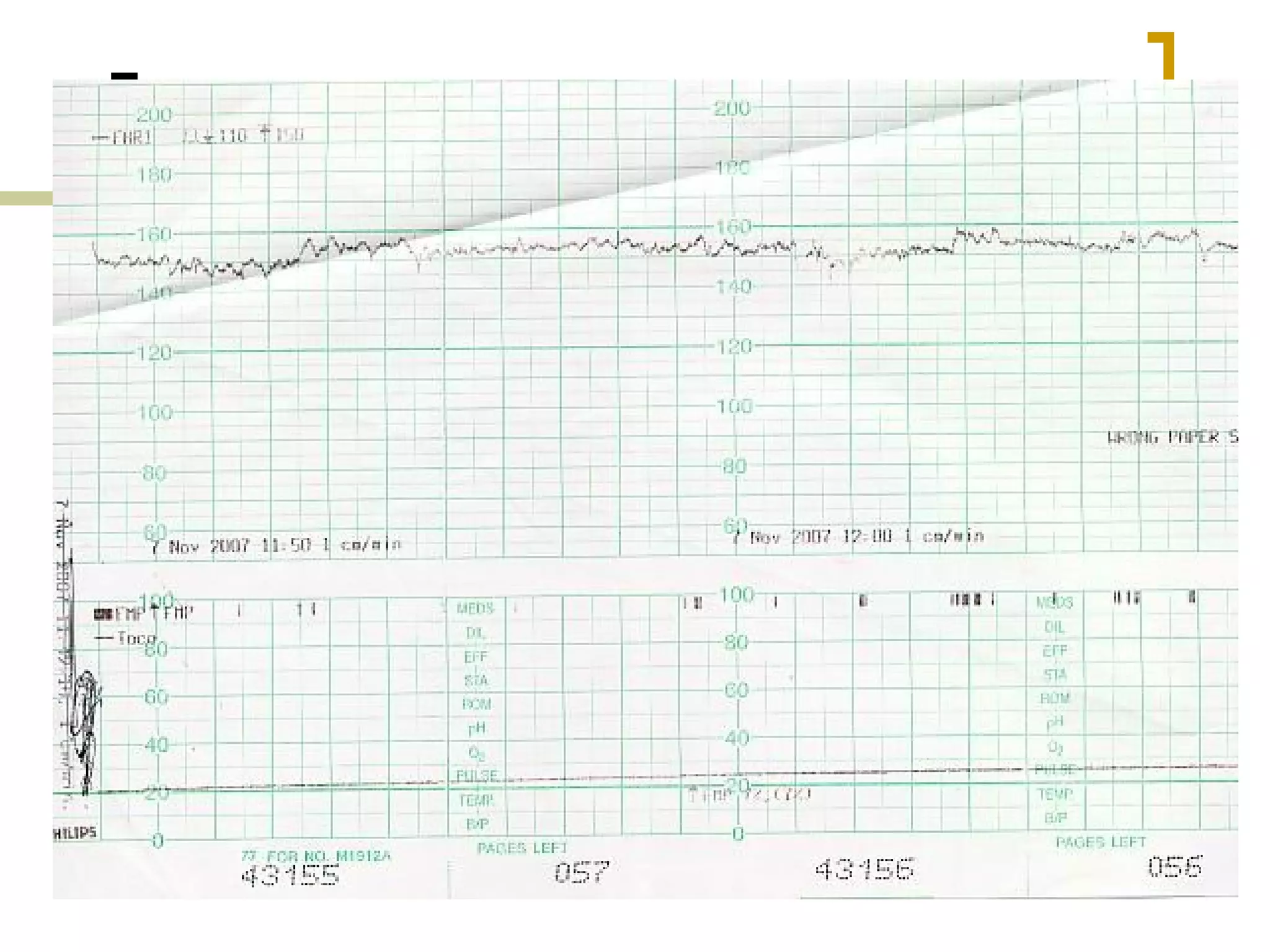
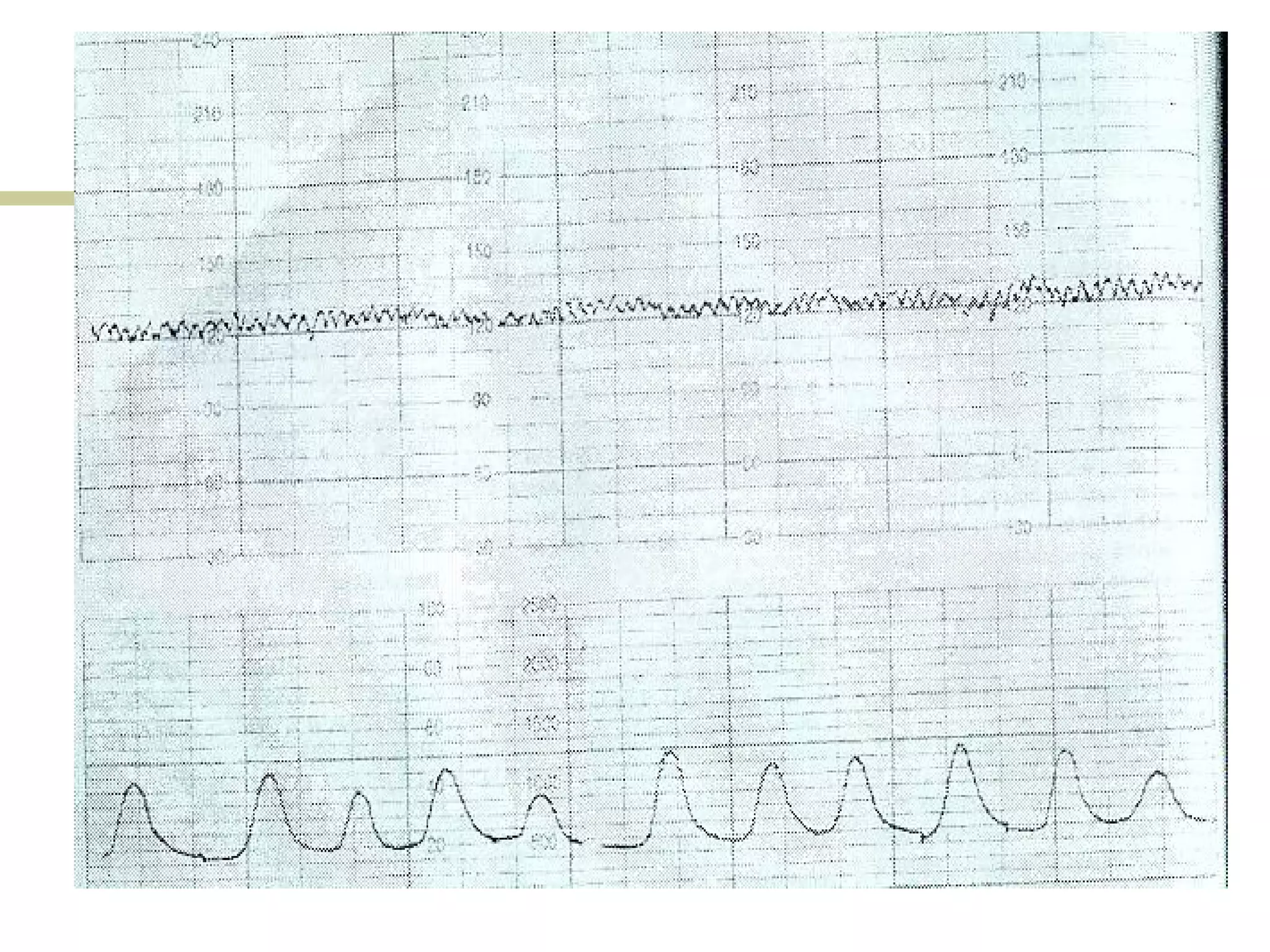
- Decreased variability, sinusoidal patterns
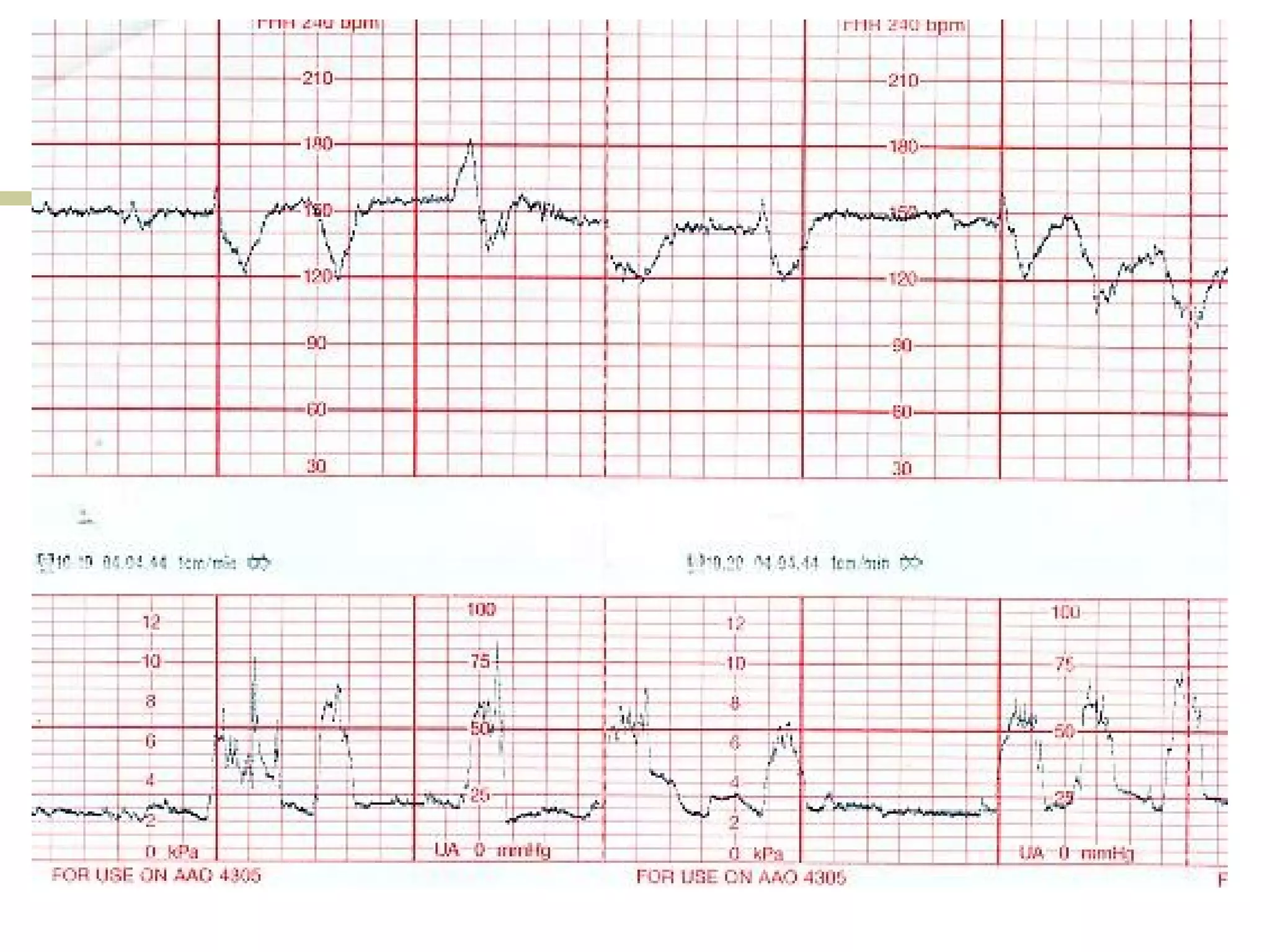
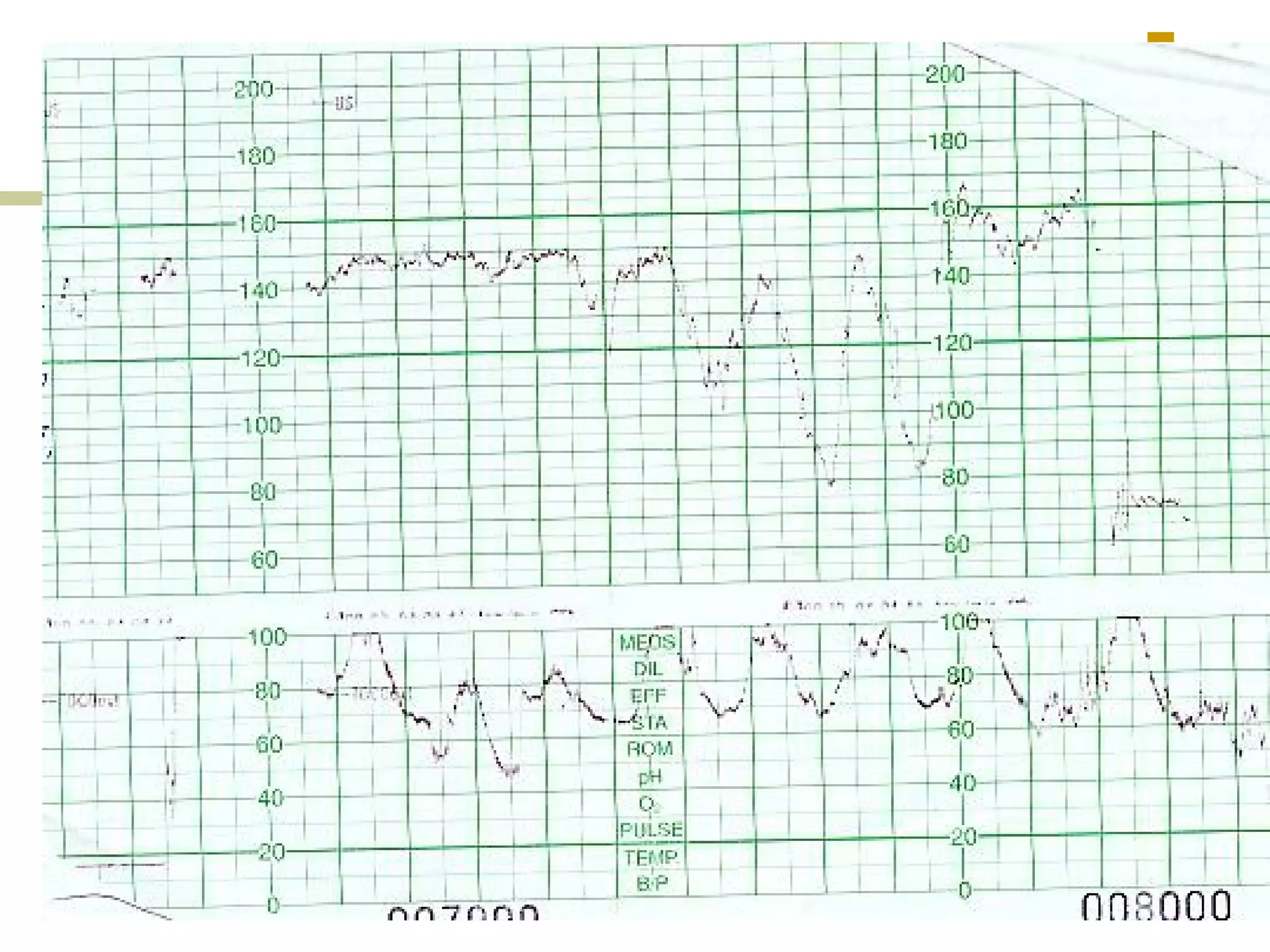
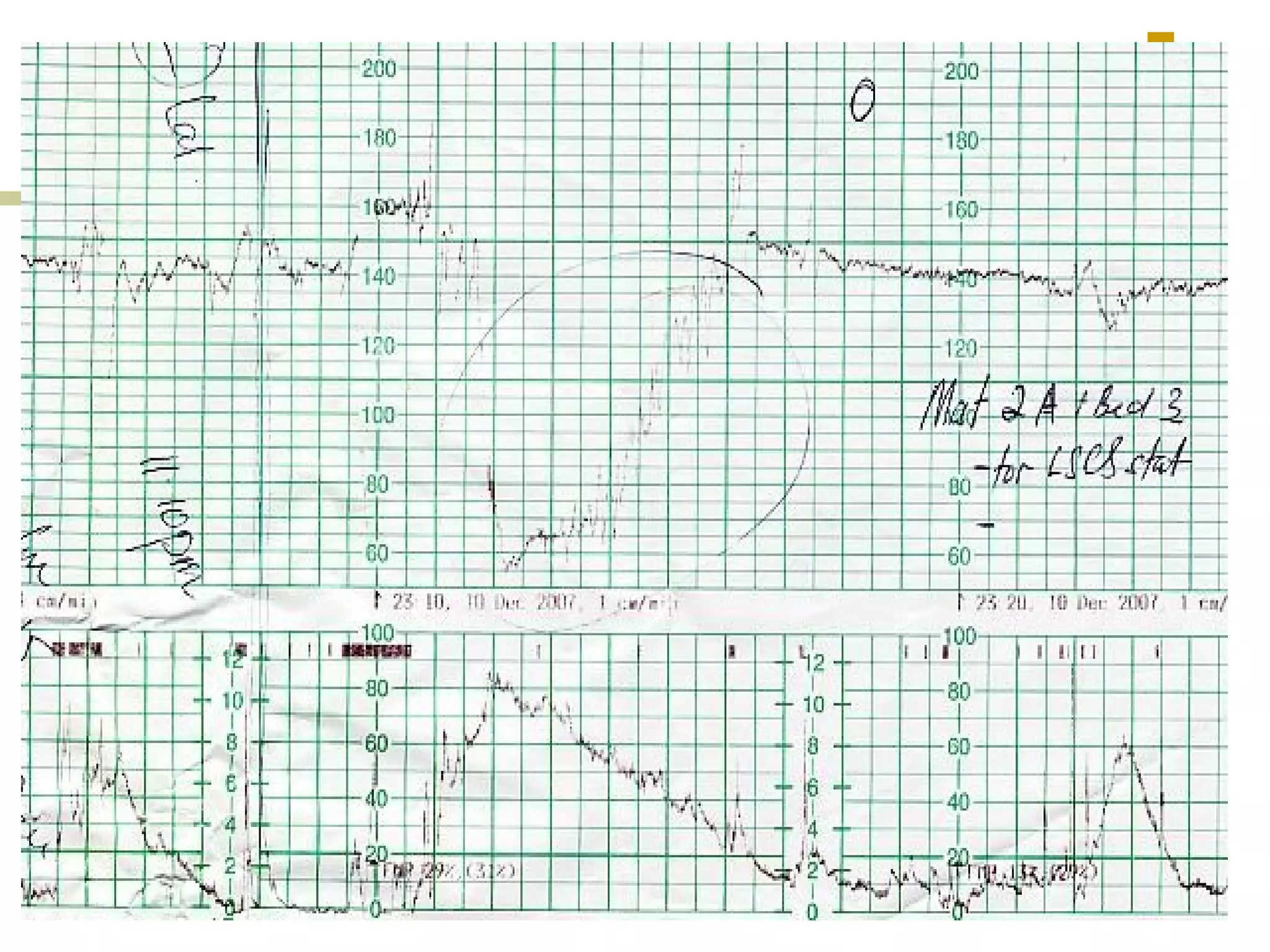
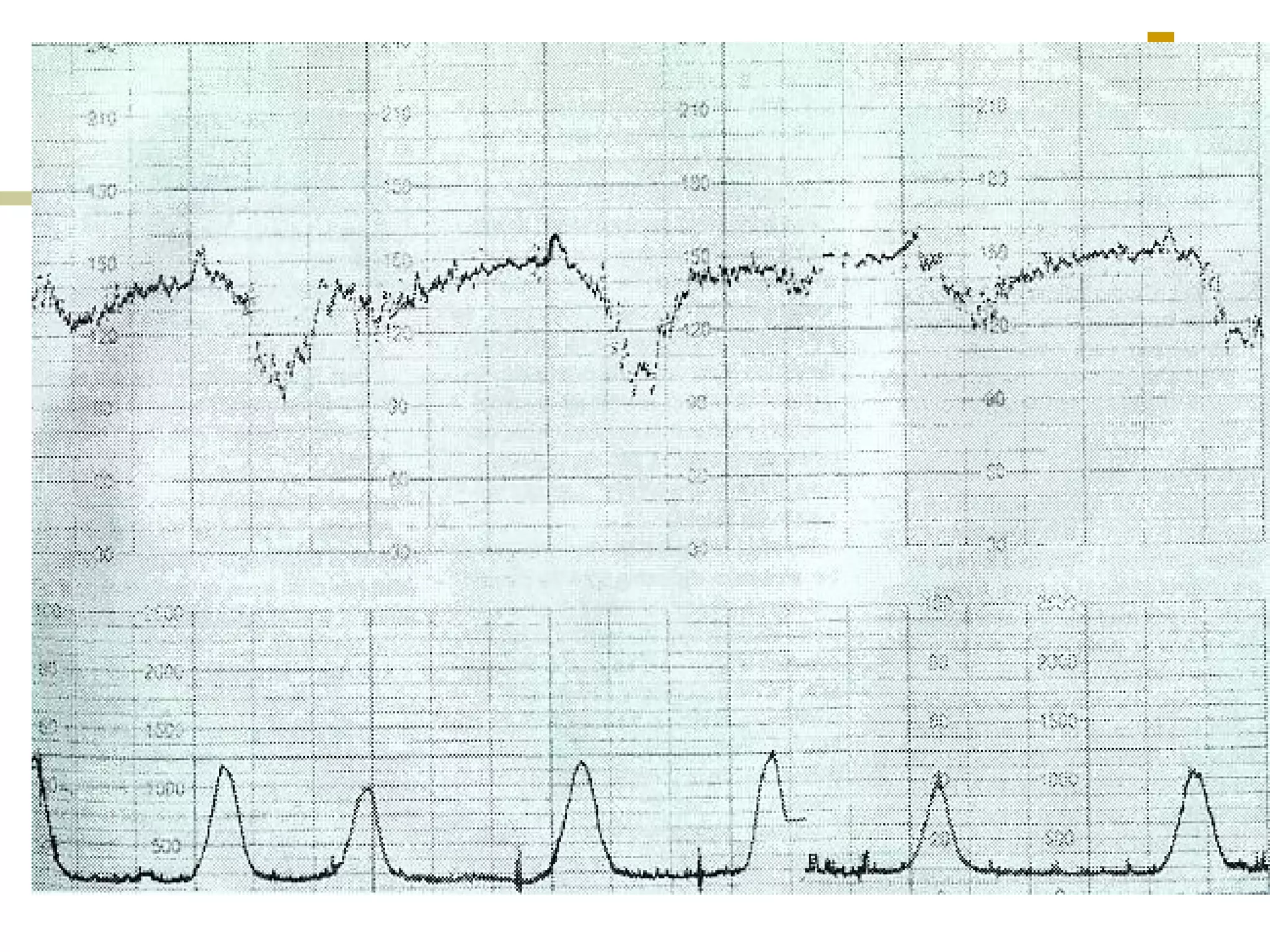
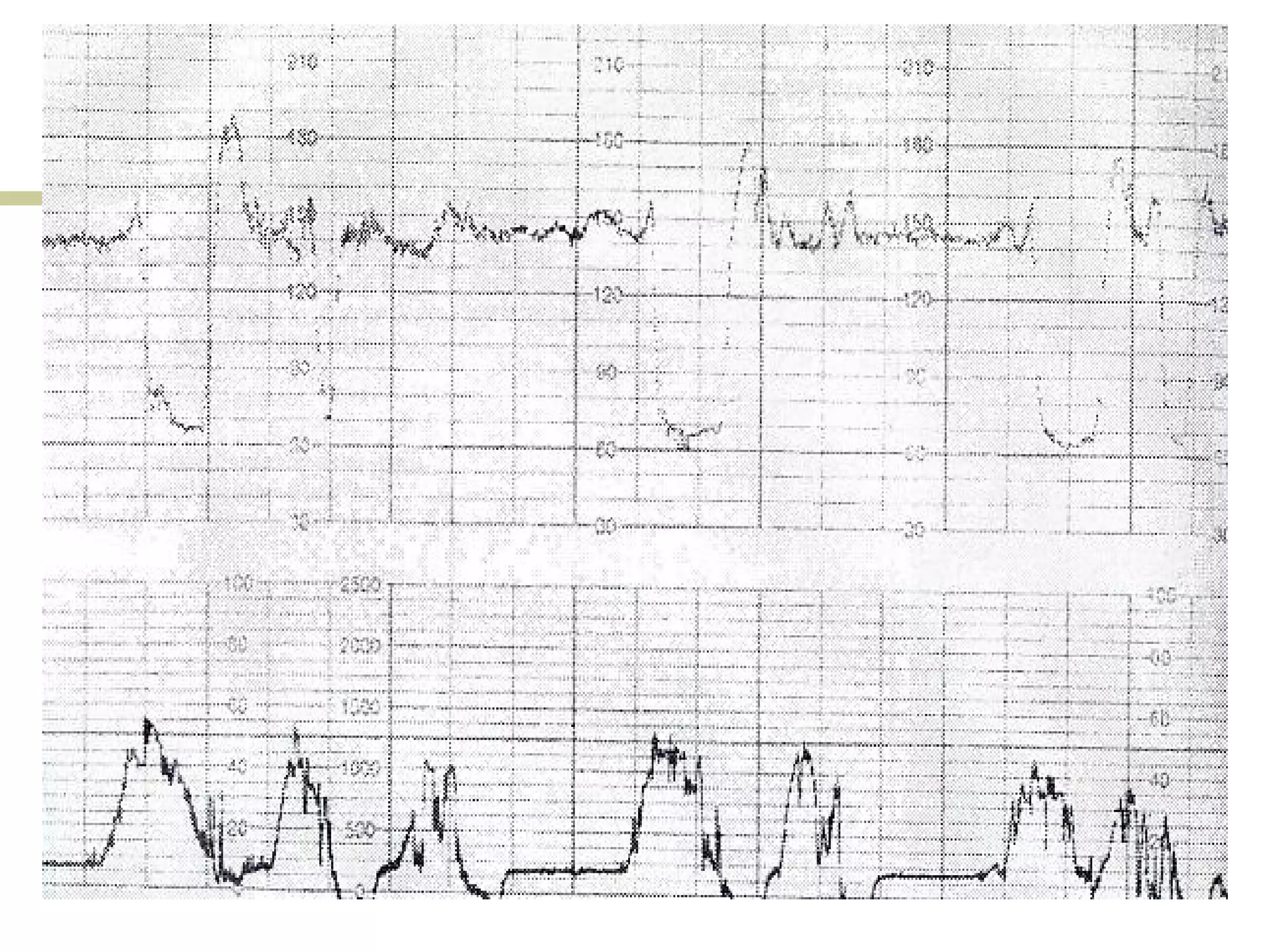
- Early, late, variable decelerations
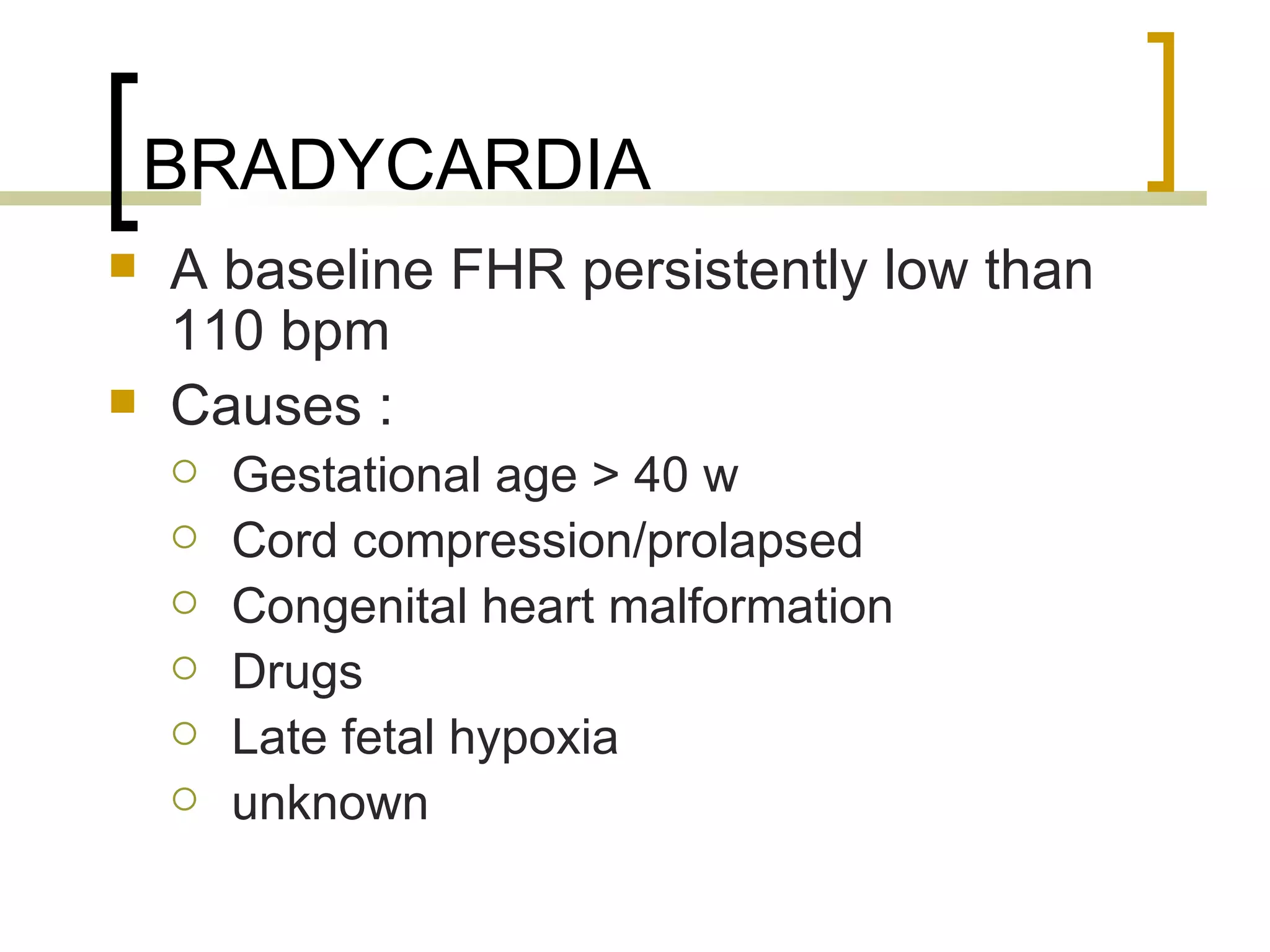
- Prolonged deceleration
- Suspicious/equivocal and pathological/ominous CTG traces
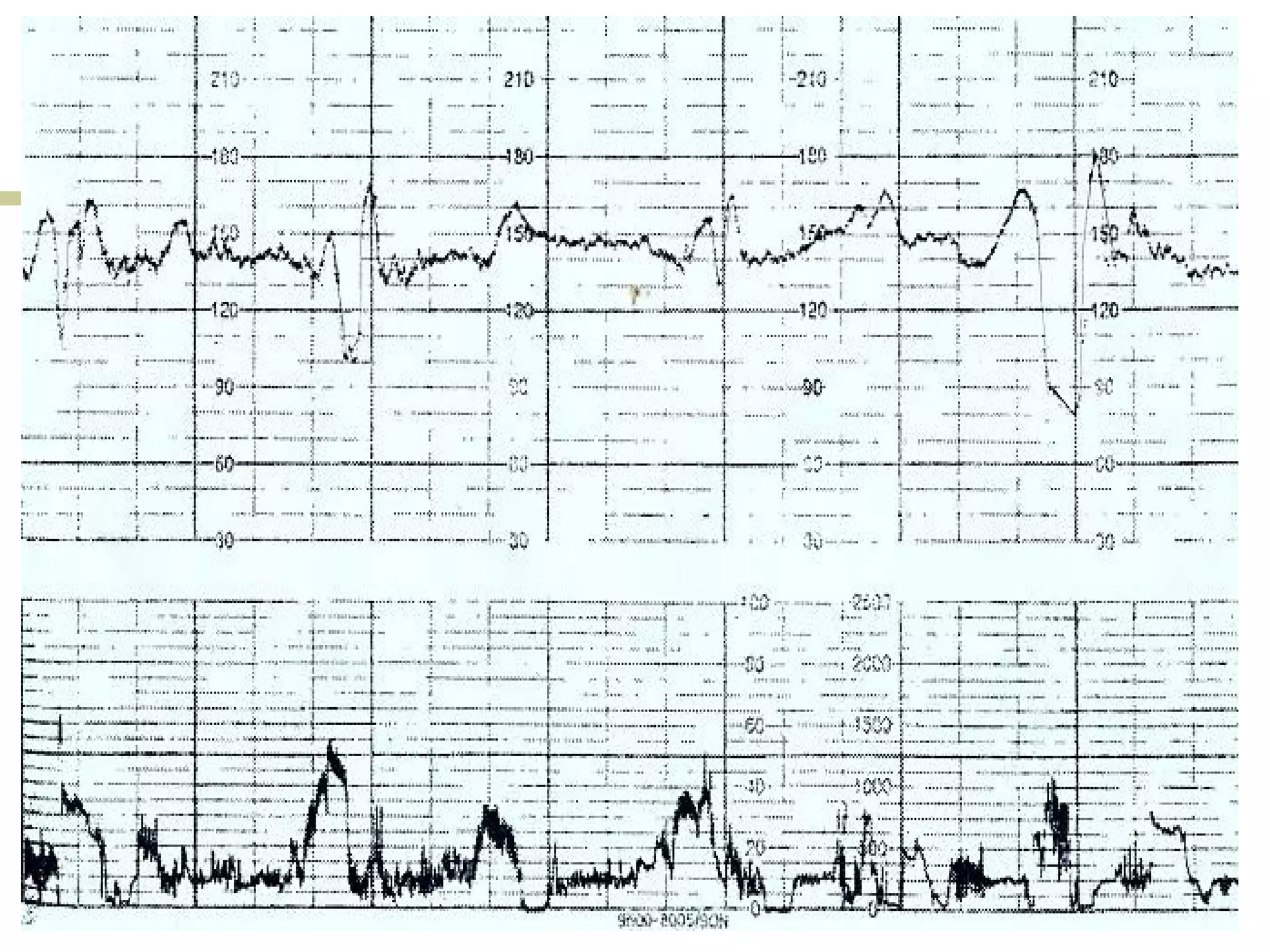
Clinical scenarios are presented involving pregnant women in labor with varying cervical dilation and fetal heart rate patterns on CTG monitoring. Uterine hyperstimulation is also defined.