Downloaded 615 times


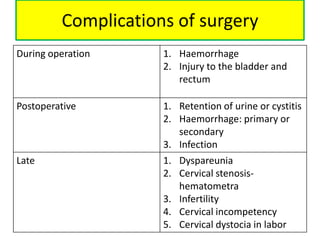

The document describes the Manchester Repair procedure, which is designed to correct uterine prolapse while preserving the uterus. The key steps are: 1) preliminary dilation and curettage of the uterus, 2) amputation of the cervix, 3) plication of the Mackenrodt's ligaments in front of the cervix, 4) anterior colporrhaphy, and 5) colpoperineorrhaphy. Additional details provided include techniques for covering the amputated cervix with vaginal flaps and suturing the Mackenrodt's ligaments to the cervix to elevate it. Potential complications of the surgery are also outlined.











































































































