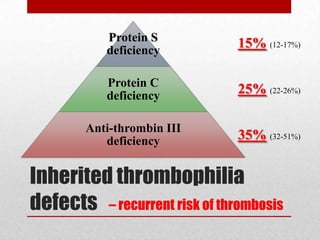
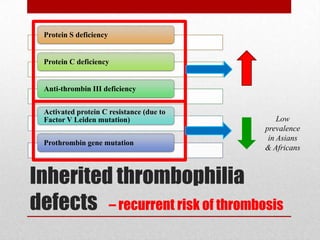
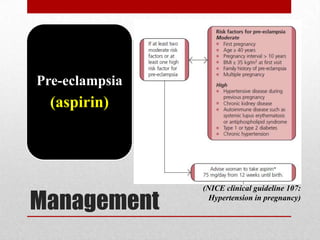
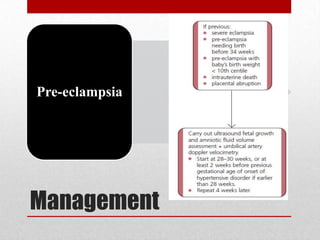
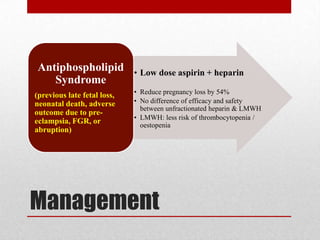
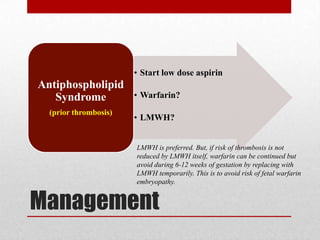
This document discusses evaluating and managing bad obstetric history (BOH). BOH refers to previous disappointments in childbearing like miscarriages, stillbirths, preterm births, or other complications. A detailed history and medical record review aims to identify recurrent or non-recurrent causes. Common causes include pre-eclampsia, inherited or acquired thrombophilia, parental genetic disorders, anatomical factors, endocrine issues, and infections. Investigation may include screening tests for these conditions. Management focuses on modifying identified risks in the current pregnancy through treatments like low-dose aspirin for pre-eclampsia risk and close monitoring throughout pregnancy. The goal is to learn from past pregnancies to optimize outcomes in future pregnancies.


















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)







