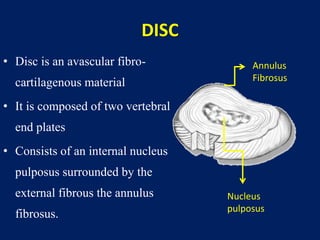
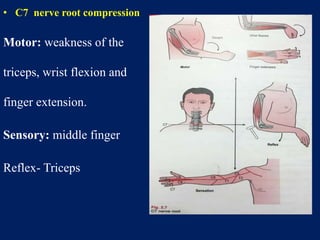
Cervical disc prolapse occurs when a cervical disc herniates and compresses the nerve root. The cervical spine has 7 vertebrae and 6 intervertebral discs that act as shock absorbers and allow motion. A disc is composed of an inner nucleus pulposus surrounded by the outer annulus fibrosus. Common sites of prolapse are C5-C6 and C6-C7. Clinical features include neck pain radiating to the arm. Imaging like MRI or CT is used to confirm prolapse. Treatment involves rest, medications, traction and surgery like anterior cervical discectomy if non-operative measures fail.